Background
Healthcare-associated infections (HAIs) are infections, which are not present at admission or might be in incubating, are acquired in the hospital (1). HAIs remain a major problem for they increase not only morbidity and mortality but also costs for health care systems. According to the recent report by the Centers for Disease Prevention and Control (CDC), about 1 in 25 U.S. hospital patients is diagnosed with at least one infection related to hospital care, with additional infections occurring in other healthcare settings (2).
Medical devices may spread infection in clinical settings (1). Devices like catheters or ventilators used in medical procedures can be contaminated by health care workers (HCWs) who have handled their cellular phones (3-8). Cellular phones used by surgical teams in operating rooms have been reported to carry pathogens and may serve as reservoirs for pathogens (4). Several viral pathogens (Respiratory Syncytial Virus, Adenovirus and Influenza Virus) have been reported in 10% of the sampled phones used by HCWs in a pilot study from Israel (5). Though pathogens may be passed by HCWs who use cellular phones, no clear association between contamination of cell phones and HAIs has been established.
This study aimed to investigate pathogenic contamination on healthcare workers’ cellular phones, detect factors associated with contamination, and demonstrate whether there was a link between cell phone contamination and subsequent HAIs.
Materials and Methods
Setting
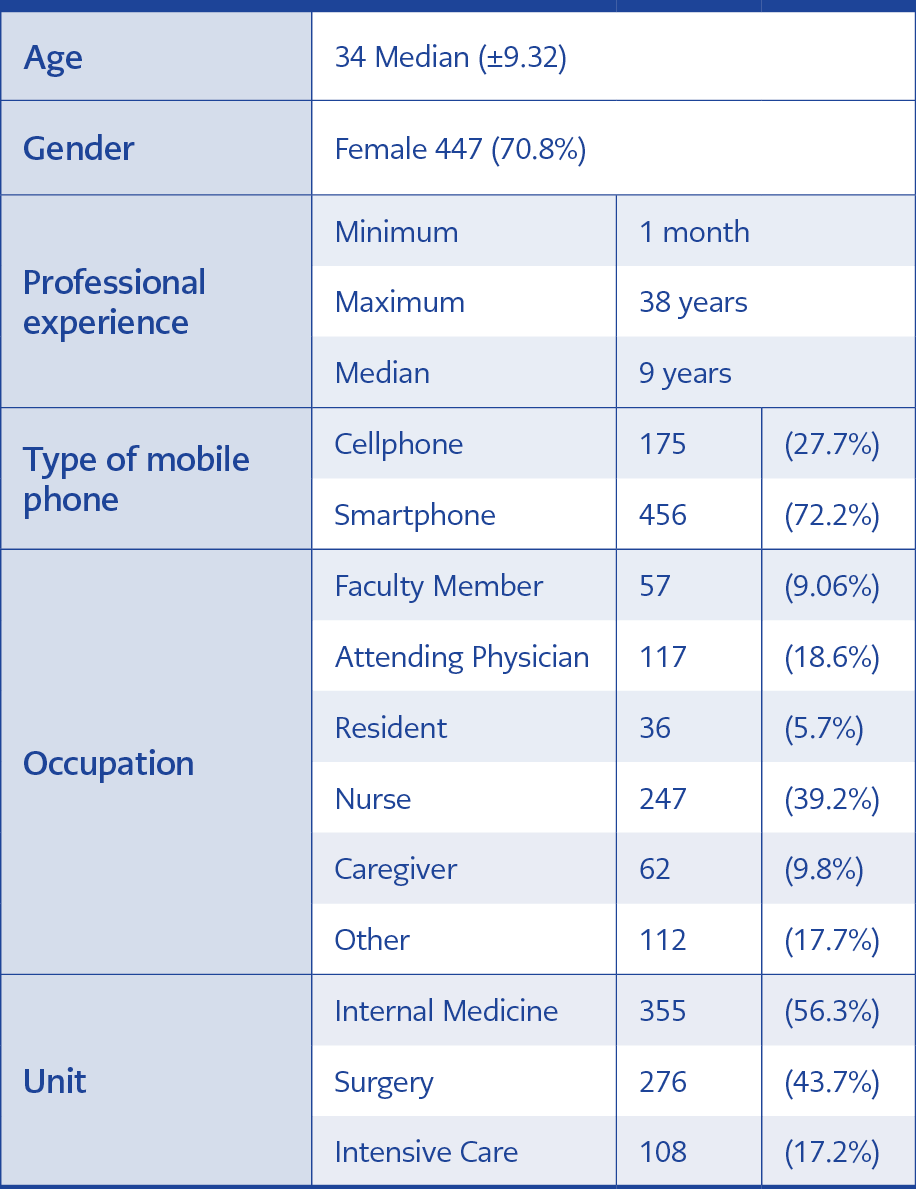
Table 1. General Features of Participants (N=631)
The study was conducted in a 2000-bed tertiary care university hospital in Ankara, Turkey. All HCWs in the hospital were invited to attend the study. A total of 631 HCWs from several departments willing to participate were included in the study (Table 1). This study was approved by Ankara University’s Committee of Research, Ethics and Deontology.
Data Collection
During study period (three weeks), bacterial cultures were taken from each cell phone. A sterile swab moistened with sterile physiological saline solution was rotated over both sides of the phone surface and cover. Obtained samples were taken to the bacteriology laboratory within one hour and streaked onto 5% sheep blood agar. Isolated microorganisms were categorized as Gram-negative or -positive by using Gram stain. Gram-negative microorganisms were identified with conventional biochemical methods (Three Sugar Iron, Indole Motility Urease, and oxidase tests) and Gram-positive microorganisms were identified with catalase and coagulase tests. Bacteria constituting skin flora (such as coagulase-negative staphylococci, Corynebacterium spp., alpha-hemolytic streptococci) were considered non-pathogenic, while bacteria other than skin flora elements were considered pathogenic. Antimicrobial susceptibility testing for pathogen bacteria was performed by disc diffusion method based on The Clinical & Laboratory Standards Institute (CLSI) guideline.
A questionnaire was performed on HCWs to collect personal information such as age, gender, occupation and current employment unit. The type of cell phone, frequency and reasons (phone call, message, social media, game, taking photo/video) for use, frequency and method of cleaning, cover, and carbon film usage were also asked in the questionnaire.
Cellular phones with a touch screen are defined as smartphones, while phones without a touch screen are defined as mobile phones.
Statistical Analysis
Data obtained from laboratory and questionnaire were analysed via a statistical software programme (STATA 9.0, TexasUSA). Chi-square test and Student’s t-test were performed to compare categorical and continuous variables, respectively. Univariate analyses were followed by logistic regression for parameters that were determined as statistically significant. Statistical significance was set as p <0.05.
Results
General features of participants and cellular phones they use are presented in Table 1.

Table 2. Pathogenic bacteria isolated from mobile phones of the 631 HCWs
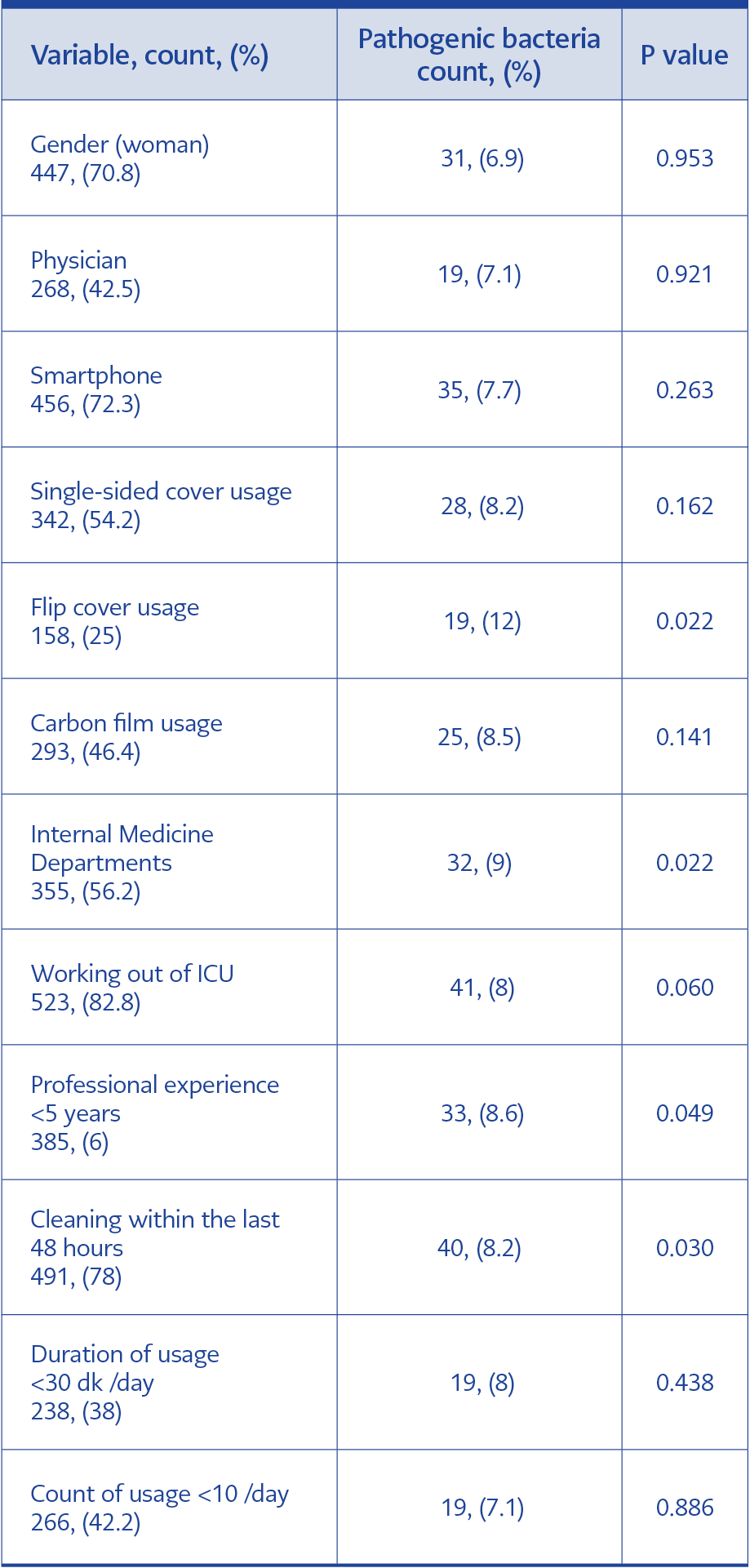
Table 3. Factors associated with pathogenic bacteria contamination (univariate analysis).
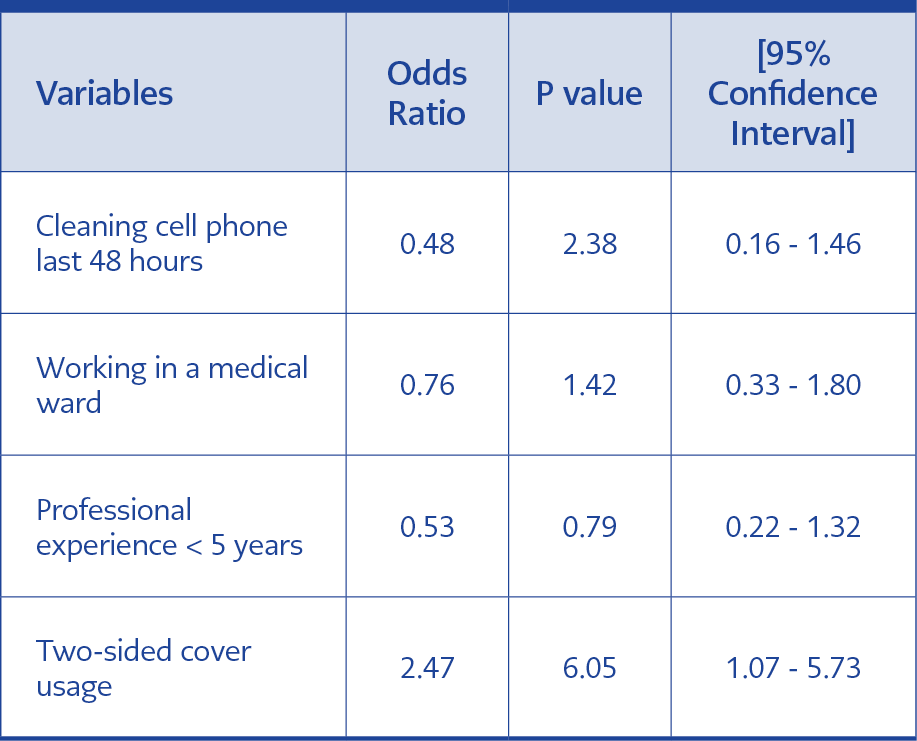
Table 4.Multivariate analysis of factors associated with pathogen contamination
All 631 cell phones investigated were contaminated with bacteria; forty-four of which were pathogenic microorganisms (Table 2) and the rest were skin flora bacteria. Drug resistance was not detected among pathogenic bacteria. Table 3 shows the variables and their association with pathogenic bacteria contamination. As determined by univariate analysis, using flip cover (P = 0.022), a professional experience of fewer than five years (P = 0.049), having cleaned the phone within the last 48 hours (P = 0.030), and working in a medical ward (P = 0.022) were significantly associated with pathogen contamination on the devices. Pathogen contamination on smartphones (7.7%) seemed to be higher than on mobile phones (5.2%). However, this difference was not statistically significant (P = 0.263). Multivariate analysis (Table 4) with logistic regression revealed that using flip cover (Figure 1) is the only factor associated with pathogen contamination on cell phones (OR:2.47; 95%CI:1.07-5.73; P=0.035) .
Discussion
In the very first study on the incidence of bacterial contamination of cellular phones, Brady et al. reported evidence of bacterial contamination, of which nearly 15% were known to cause HAIs. Based on the assumption that the use of cell phones in hospitals may not be restricted, the authors recommended working on decontamination methods such as the use of alcohol disinfectant wipes in order to avoid cross-infection in healthcare settings (6). Indeed, several other studies documented that decontamination with alcohol reduced contamination (9-11). We did not evaluate the efficiency of decontamination. However, having cleaned the phone within the last 48 hours resulted in lower rates of contamination. As for medical devices, a specific decontamination procedure for cell phones seems inevitable in the near future, considering the extensive use of cell phones.
Suganya S. et al. (2012) reported that wiping the cell phones with 95% ethanol and covering them with plastic cover reduced bacterial growth by nearly 90% (9). Their data is not comparable to ours since we evaluated the effect of the flip covers, which are protective for physical damage, and found that bacterial contamination was significantly higher in those cell phones (12.03% vs. 5.08% ).
Previous studies reported a wide range of contamination rates (8% – 72%) of cell phones by pathogenic bacteria from different levels and units of health care facilities in Turkey (8, 12, 13). Optimistically, somewhat lower contamination by pathogenic bacteria (6.05%) in our study may be associated with elevated awareness based on previous experiences.
Only one study compared smartphones and mobile phones in terms of contamination (14). The authors reported that smartphones were more often contaminated by pathogenic bacteria than mobile phones (35% vs. 20%) because of larger surfaces and additional features. Although our initial hypothesis was along the same line, we did not observe a higher level of contamination in smartphones than mobile phones. Other differences -such as bacterial species- exist among studies focusing on contamination through hands and cell phones. A study from India reported that there were no contamination with Gram-negative bacteria and Enterococcus on cellular phones of HCWs (15). The authors speculated that predominant colonization of Staphylococci on the hands of HCWs might have interfered with Gram-negative species. Although coagulase-negative Staphylococcus was the dominant bacteria on cell phones, we isolated Gram-negative bacteria such as E. coli, Acinetobacter, Pseudomonas, Serratia, Providencia. In our study, none of the pathogenic bacteria showed antimicrobial resistance while VRE, MRSA, and imipenem resistant Acinetobacter strains were identified by Loyala S. et al. (16).
One of our initial goals was to investigate cross-contamination between the cellular phone and the patient. According to the data collected by the infection control team, no HAIs related to the pathogens that we isolated from the cellular phones of the HCWs throughout this study occurred. However, without further investigation, it would be rather premature to assume that cellular phones are not associated with cross-contamination. Carefully structured further research should establish if such a link exists between cellular phone use and HAIs.
Conclusion
Using a flip phone cover is a significant risk factor for the contamination of HCW mobile phones. Although we could not show any HAI occurred by the bacteria isolated from cell phones, we do not recommend health care workers using flip covers.