Introduction
The number of patients with hematological malignancies (HMs) and those undergoing hematopoietic stem cell transplantation (HSCT) has been on rise during the last three decades. Febrile neutropenia (FN) is the most common complication in this specific patient group and requires urgent intervention (1).
Bacteremia are a significant cause of neutropenic fever and severe complications in patients with HMs, causing delays in chemotherapy, longer hospitalizations, increased health care expenditures, and higher mortality and morbidity rates (2, 3). Bacteremia is generally seen in patients with prolonged and severe neutropenia, ranging from 11% to 38% depending on the use of prophylactic antibiotics (2-5). The overall mortality rates of bacteremia in patients with HMs vary from 12% to 42% (6, 7).
In recent years, changes in the epidemiology of bacteremia have been observed according to geographical regions and even between hospitals in the same location (8). Gram-negative (GN) bacteria have still been reported as the prevalent cause in recently published studies (2, 8-10). Bacteremia with resistant GN bacteria (e.g., carbapenem-resistant Enterobacterales (CRE) and multidrug-resistant (MDR) Pseudomonas aeruginosa and Klebsiella pneumoniae) have become a considerably significant problem in this fragile group (11, 12). Turkey has one of the highest bacterial resistance rates in Europe, thus this epidemiology may adversely affect the management of patients with FN (13).
In this study, we aimed to investigate the factors affecting the development of GNB and compare mortality rates among bacteremic and non-bacteremic patients with HMs with or without HSCT in a high-resistance setting.
Materials and Methods
Setting and Data Collection
This study was performed at Hacettepe University Hospitals, which is a reference center for autologous and allogeneic HSCT in Turkey. Data collected from hospital files of patients and the laboratory database included; age, gender, comorbidities, underlying HMs, treatment response, type/timing of HSCT (autologous or allogenic), graft-versus-host disease, treatment with antibiotics/steroids/monoclonal antibody within the last three months, antibiotic prophylaxis, prior hospitalization (within the last three months), prior bacteremia within the last three months, surgery and other invasive procedures, presence of central venous catheter or urinary catheter, clinical/laboratory/imaging findings, current/prior administration of chemotherapy, duration of hospitalization and neutropenia before bacteremia/febrile neutropenic episode, mucositis, radiotherapy, fever and shock on presentation, need for intensive care unit (ICU) or mechanical ventilation, number of positive blood cultures, microorganisms and their susceptibility profiles, colonization with resistant microorganisms, empirical antibiotic treatments, appropriateness of empirical therapy, definitive antibiotic treatment, the source of infections, clinical outcomes and mortality. The collected data were entered into a specific database designated for this study.
Study Population and Design
We conducted a prospective cohort study to identify predictors associated with GNB and 30-day mortality among febrile neutropenic patients aged ≥18 years with HMs. For this study, we followed up 66 bacteremic and 132 non-bacteremic patients with HMs from March 2018 to June 2019. Additionally, we analyzed the trends in antimicrobial resistance (AMR) in 276 GN bacteria isolates which have been screened between January 2010-June 2019. Recurrent episodes of bacteremia for the same patient were excluded.
Definitions
Neutropenia was defined as an absolute neutrophil count of <500 cells/mm3 (1). Sepsis was defined as having a systolic pressure <90 mmHg with dysregulated host response to infection. Septic shock was characterized as sepsis associated with hypotension and perfusion abnormalities despite adequate fluid replacement or the need for vasoactive drugs (14). Bacteremia was defined as laboratory-confirmed isolation of at least one GN bacteria from blood samples in a patient with signs/symptoms of infections (15). If the source of bacteremia was unknown, this was named primary bacteremia, if known this was named secondary bacteremia.
Enterobacterales and non-fermenting GN bacteria including P. aeruginosa, Acinetobacter baumannii, and Stenotrophomonas maltophilia were considered to be MDR or extensively drug-resistant (XDR) according to the previously described criteria (16).
Appropriate empirical therapy was considered when the patient received at least one in vitro active antimicrobial agent before susceptibility results were available. Death was considered to be related to the bacteremia if it occurred before the resolution of symptoms or signs and there was no other explanation. In accordance with the local protocol, patients with expected neutropenia over seven days received prophylaxis with a fluoroquinolone.
Microbiological Methods
Blood samples were analyzed with the BACTEC™ 9240 (Becton–Dickinson, USA) until 2012, with the BacT/ALERT® 3D system (bioMérieux, France) between 2013-2017 and BACTEC™ FX (BD Diagnostics, USA) thereafter, with an incubation period of 5 days.
Microbial identification was performed by using BD Phoenix™ system (Becton-Dickinson, USA) until 2012. From 2013 to 2017, isolate identity was confirmed by Vitek® MS (bioMérieux, France) and as of 2018 by MALDI Biotyper® (Bruker Daltonics, USA).
Minimum inhibitory concentrations (MICs) were determined by BD Phoenix™ system (Becton-Dickinson, USA) until 2012, Vitek® 2 Compact automated system (bioMérieux, France) during 2013–2017 and BD Phoenix™ M50 (Becton-Dickinson, USA) thereafter.
Kirby-Bauer disk diffusion test was used for the determination of antimicrobial susceptibilities of the non-fermenting GN bacteria, except P. aeruginosa. Gradient test (bioMérieux, France) was used for the confirmation of carbapenem resistance according to the manufacturer’s instructions. The susceptibility of isolates for colistin was performed by using Sensititre™ broth microdilution panels (Thermo Fisher Scientific, USA).
Before 2017, all results were interpreted according to the Clinical and Laboratory Standards Institute (CLSI) and after 2017 according to European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines.
Quality assurance was performed by concurrently testing CLSI-recommended quality control (QC) reference strains (Escherichia coli ATCC 25922, Staphylococcus aureus ATCC 25213). All QC results were within published acceptable ranges.
Statistical Analysis
Values were expressed as the means ± standard deviations and median and interquartile range (IQR) for continuous variables, whereas nominal variables were presented as numbers and percentages. Variables in this study were selected based on theoretically based hypotheses, together with the results demonstrated in previous studies. Continuous variables were compared by Student’s t-test or Mann-Whitney U test. Categorical variables were evaluated with Pearson’s chi-square or Fisher’s exact test. Odds ratios and 95% confidence intervals were calculated to assess the strength of any association. The statistical significance was defined as a p value of <0.05. Variables associated with GNB and mortality in univariate analysis (p≤0.10) were included in the backward stepwise logistic regression model to identify independent factors for GNB and mortality. The Hosmer-Lemeshow test assessed the goodness of fit of the multivariate models. Variables were not included in the regression model when p values were highly significant or had a positive correlation with other variables. The Kruskal-Wallis test was used to calculate the ratios between resistance profiles that changed between years. The Jonckheere-Terpstra test was used to evaluate the changing trends between these ratios. The Statistical Package for Social Sciences (SPSS) version 24.0 (IBM Corp., USA) was used for all statistical analysis.
Results
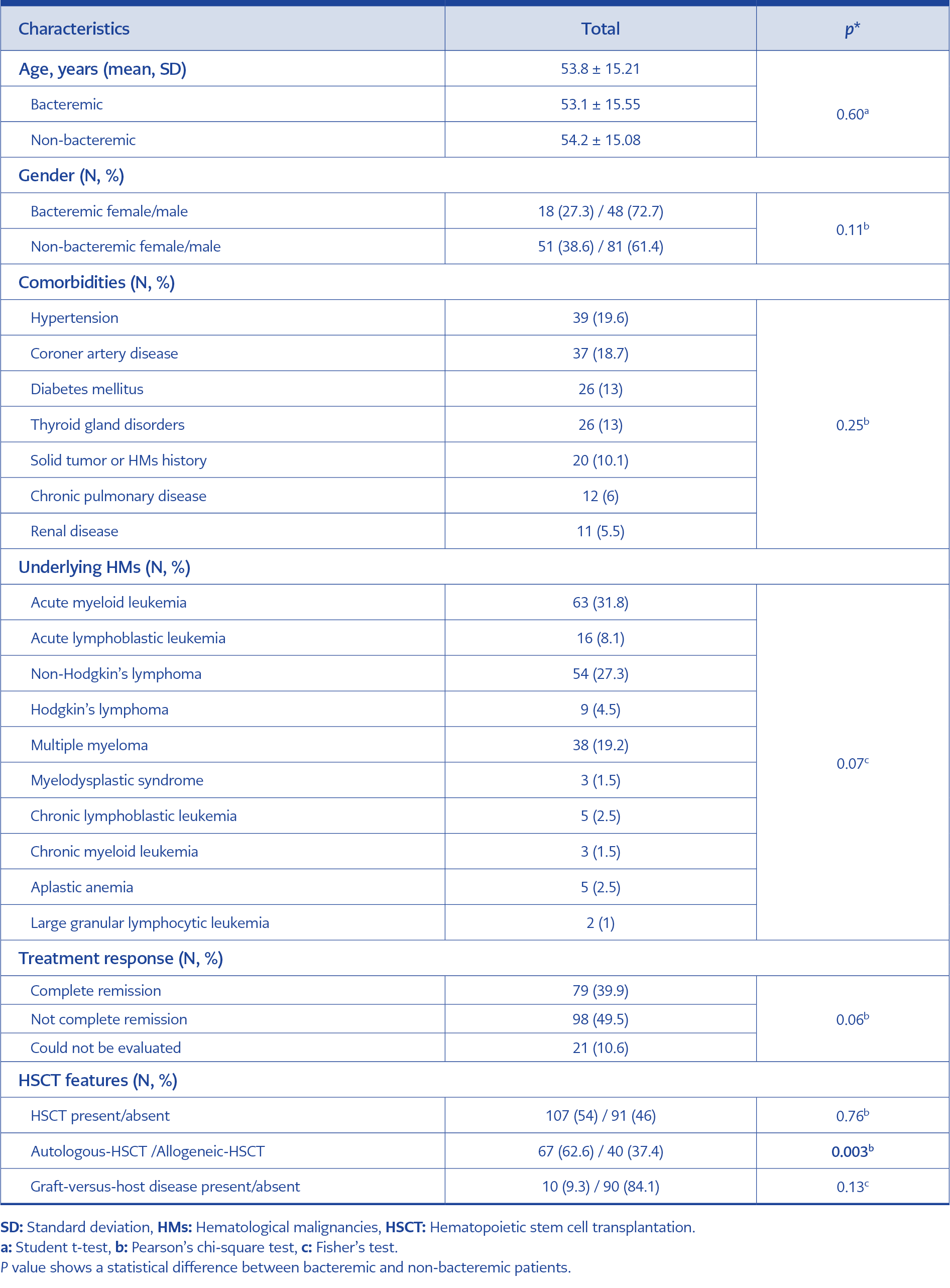
Table 1. Basic demographics of the patients.
Data of 66 bacteremic and 132 non-bacteremic controls with HMs were analyzed. One hundred and twenty-nine (65.2%) of the patients were male. The mean age was 53.83±15.21 years (Table 1).
The patients were stratified into three groups according to their underlying malignancies and/or HSCT status as follows:
Group 1: Leukemias (acute myeloid and lymphocytic leukemia) and allogeneic transplant recipients,
Group 2: Lymphomas (Non-Hodgkins’s and Hodgkin’s lymphoma),
Group 3: Others (multiple myeloma, chronic myeloid and lymphocytic leukemia, large granular lymphocytic leukemia, myelodysplastic syndrome, aplastic anemia).
There was a significant difference between the number of bacteremic and non-bacteremic patients in these three groups (p=0.001). Post-hoc analysis showed that the difference was due to the higher rate of bacteremia in leukemia and allogeneic transplant recipients.
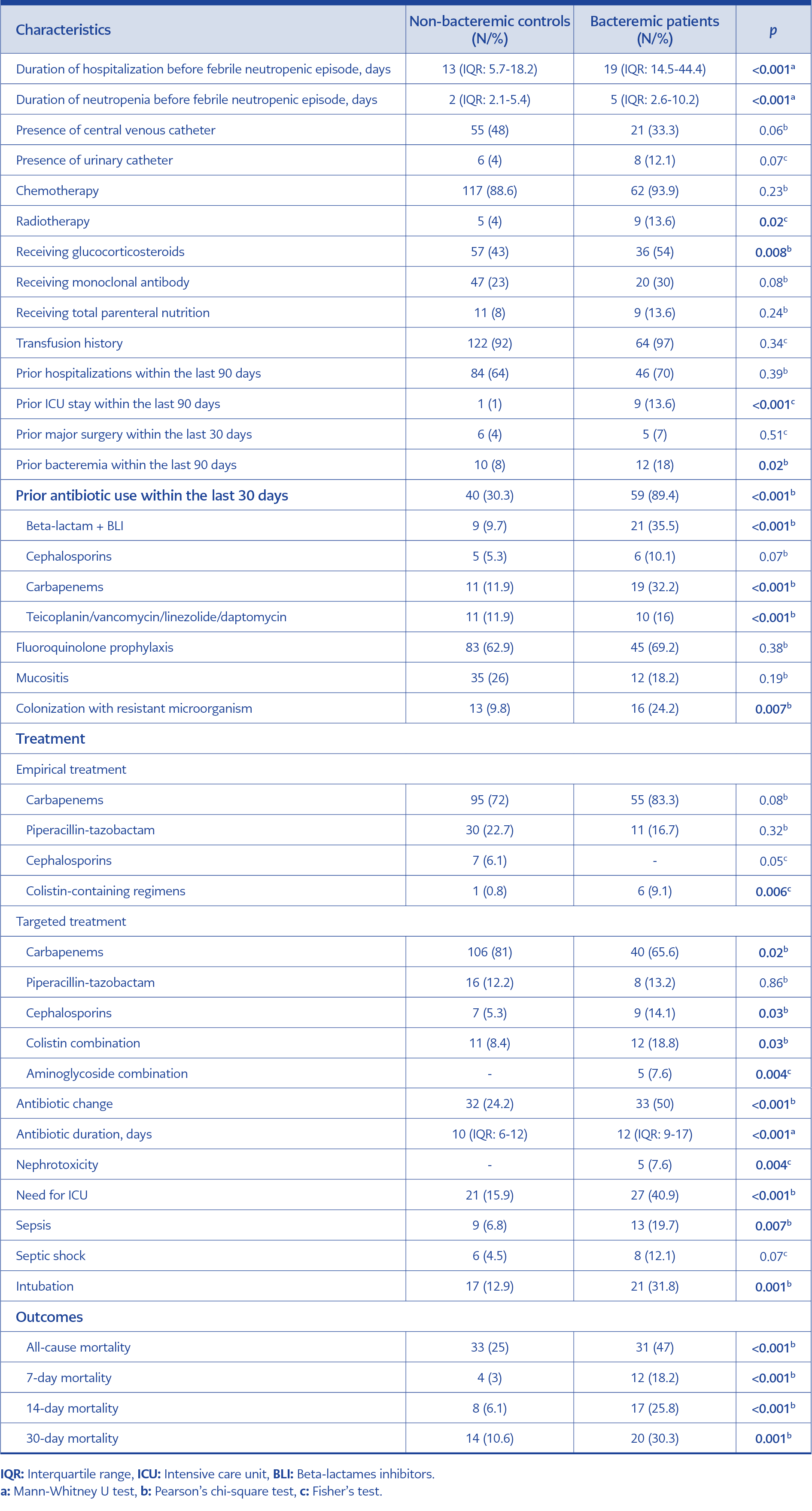
Table 2. Comparison of characteristics in bacteremic patients to non-bacteremic controls.
When bacteremic and non-bacteremic patients were compared, the duration of hospitalization and neutropenia before the febrile neutropenic episode were both longer in the former group (19 [IQR:14.5-44.4] vs 13 [IQR: 5.7-18.2] days and 5 [IQR: 2.6-10.2] vs 2 [IQR: 2.1-5.4] days respectively). Prior antibiotic exposure particularly to beta-lactamase inhibitor combinations and carbapenems during the past 30 days was more frequent in the bacteremic group (Table 2).
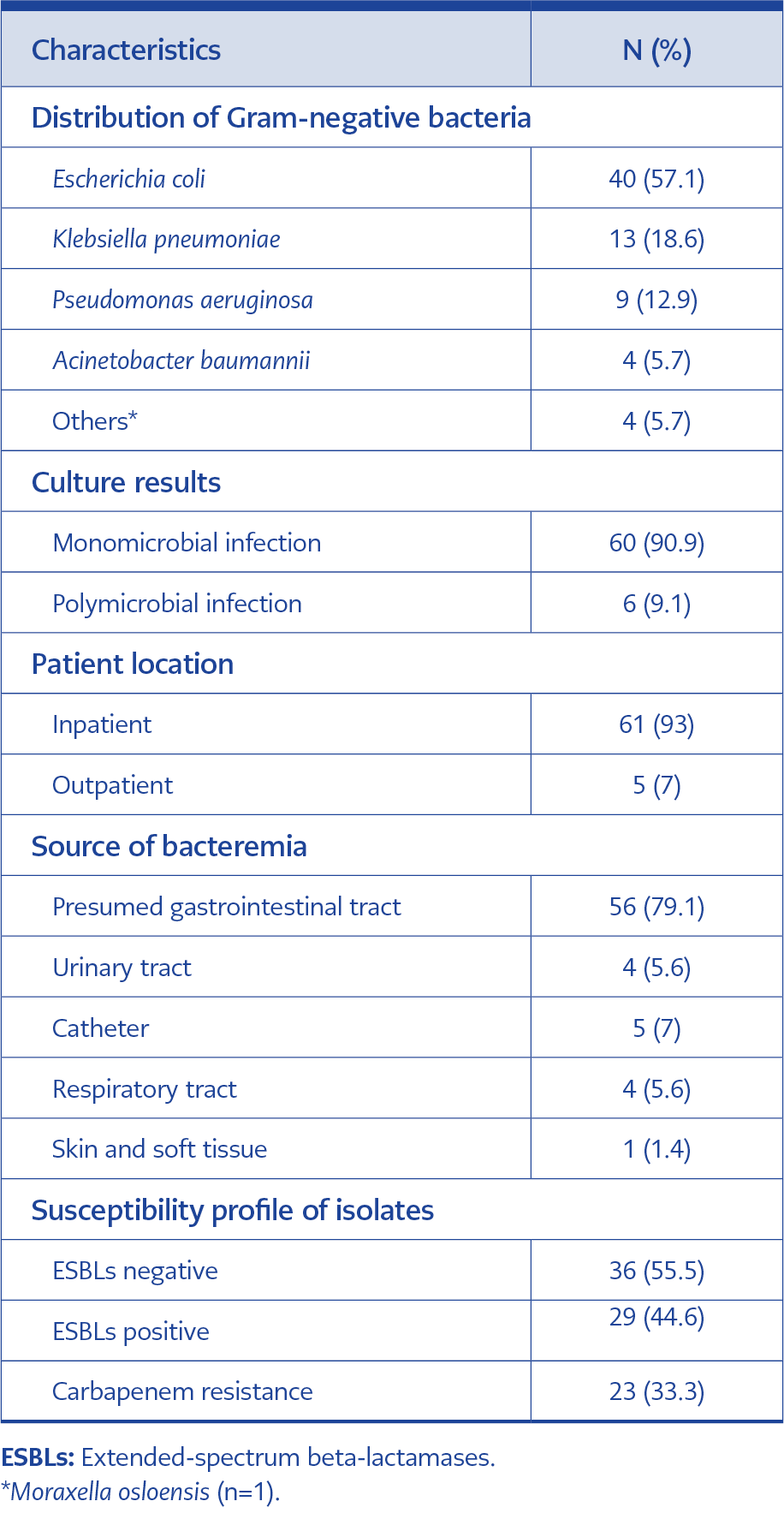
Table 3. Microbiological characteristics of bacteremic patients.
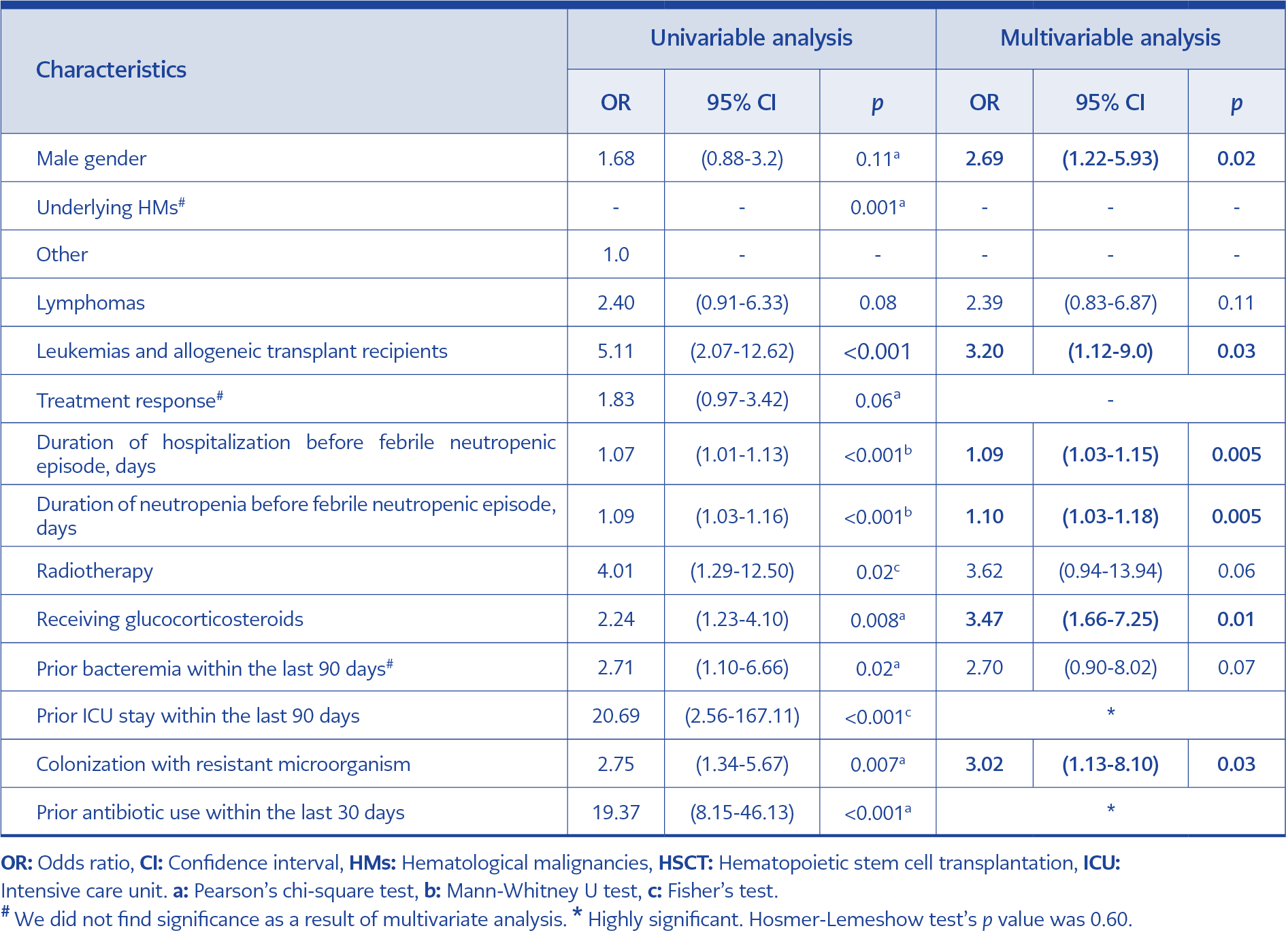
Table 4. Univariable and multivariable analysis of factors associated with GN bacteremia in neutropenic patients compared to non-bacteremic controls.
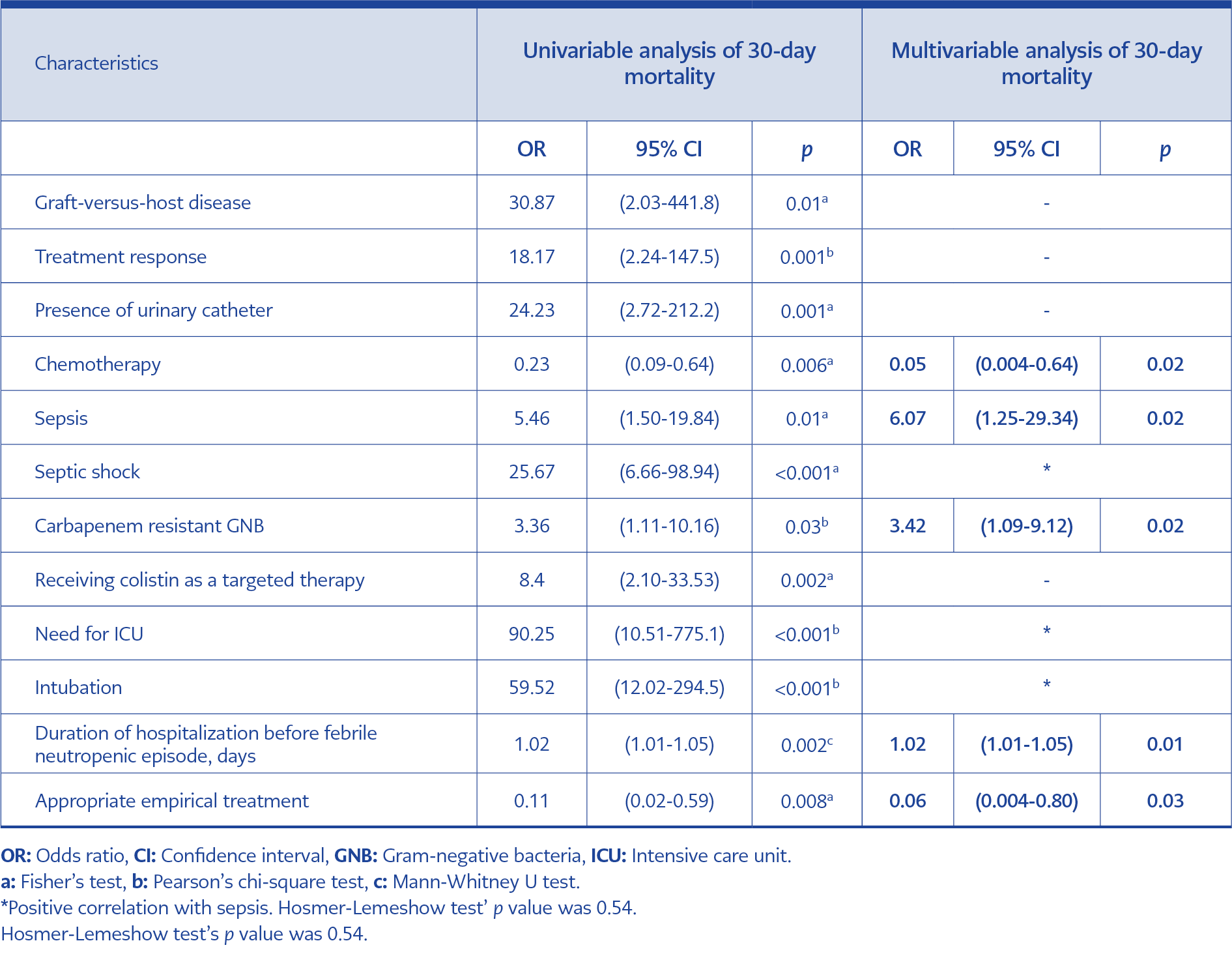
Table 5. Univariable and multivariable analysis of factors associated with 30-day mortality in bacteremic patients.
Seventy GN bacteria caused 66 bacteremic episodes. The majority of bacteremic episodes were monomicrobial (n=60, 90.9%). E. coli was the most common species (n=40; 57.1%). Polymicrobial episodes included isolation of two different bacteria (E. coli + P. aeruginosa in two patients, E. coli + K. pneumoniae in two patients, E. coli + Enterococcus faecium in one patient and P. aeruginosa + Clostridium spp. in one patient) (Table 3).
In 13.6% of the bacteria, production of extended-spectrum beta-lactamases (ESBLs) and carbapenem resistance were detected concurrently. The initial empirical antibacterial treatment was appropriate in 58 (87.9%) patients. More antibiotic changes were made in bacteremic patients as compared with non-bacteremic controls (The antibiotic change was made in 33 (50.0%) of 66 bacteremic patients (50.0% vs 24.2%, p<0.001) (Table 2). The reasons for the change in bacteremic cases were de-escalation in 16 (24.2%) patients; clinical failure in 7 (10.6%); suspected other infections in 5 (7.6%) side effects in 1 (1.5%) replaced due to and in-vitro resistance in 4 (6.1%). In the control group, antibiotic changes were made per clinical and laboratory results and suspicion of other infectious foci.
Six (9.1%) of 66 patients with bacteremia never received active antibiotic treatment because they died before the availability of susceptibility results. Prolonged meropenem infusion was administered in 16 (8.1%) patients.
All-cause mortality was 47.0% vs 25.0% in cases of GNB, compared to non-bacteremic controls (p<0.001). Seven-day mortality was also higher in cases of GNB (18.2%) than in the control group (3.0%, p<0.001). Fourteen-day and thirty-day mortality were 25.8% and 30.3% in cases of GNB and, 6.1% and 10.6%, in non-bacteremic controls, respectively (p<0.001, p=0.001) (Table 2).
Univariable and multivariable analysis of factors associated with 30-day mortality in bacteremic patients were shown in Table 5.
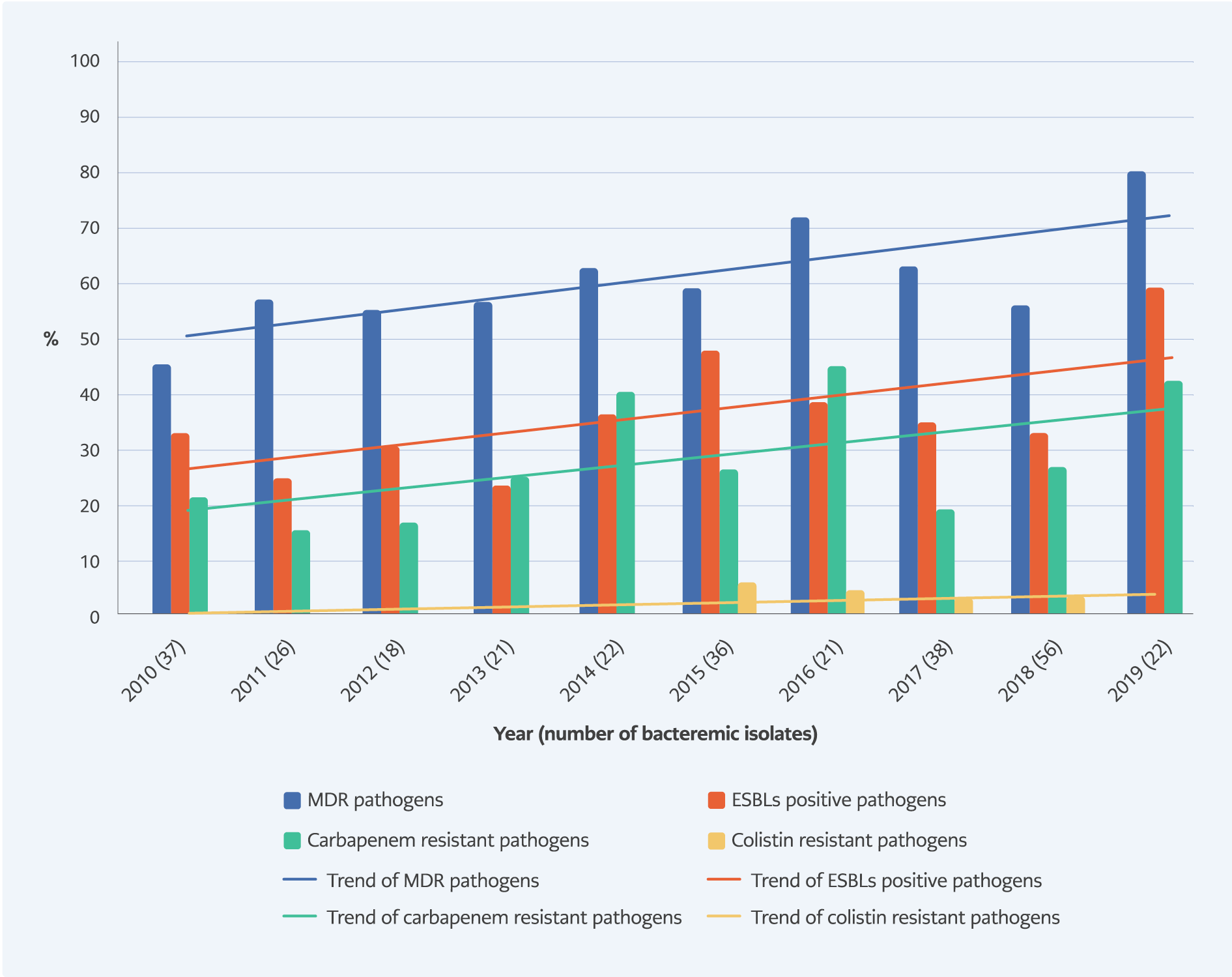
Figure 1. Antimicrobial resistance profiles in gram-negative bacteria between 2010 and 2019.
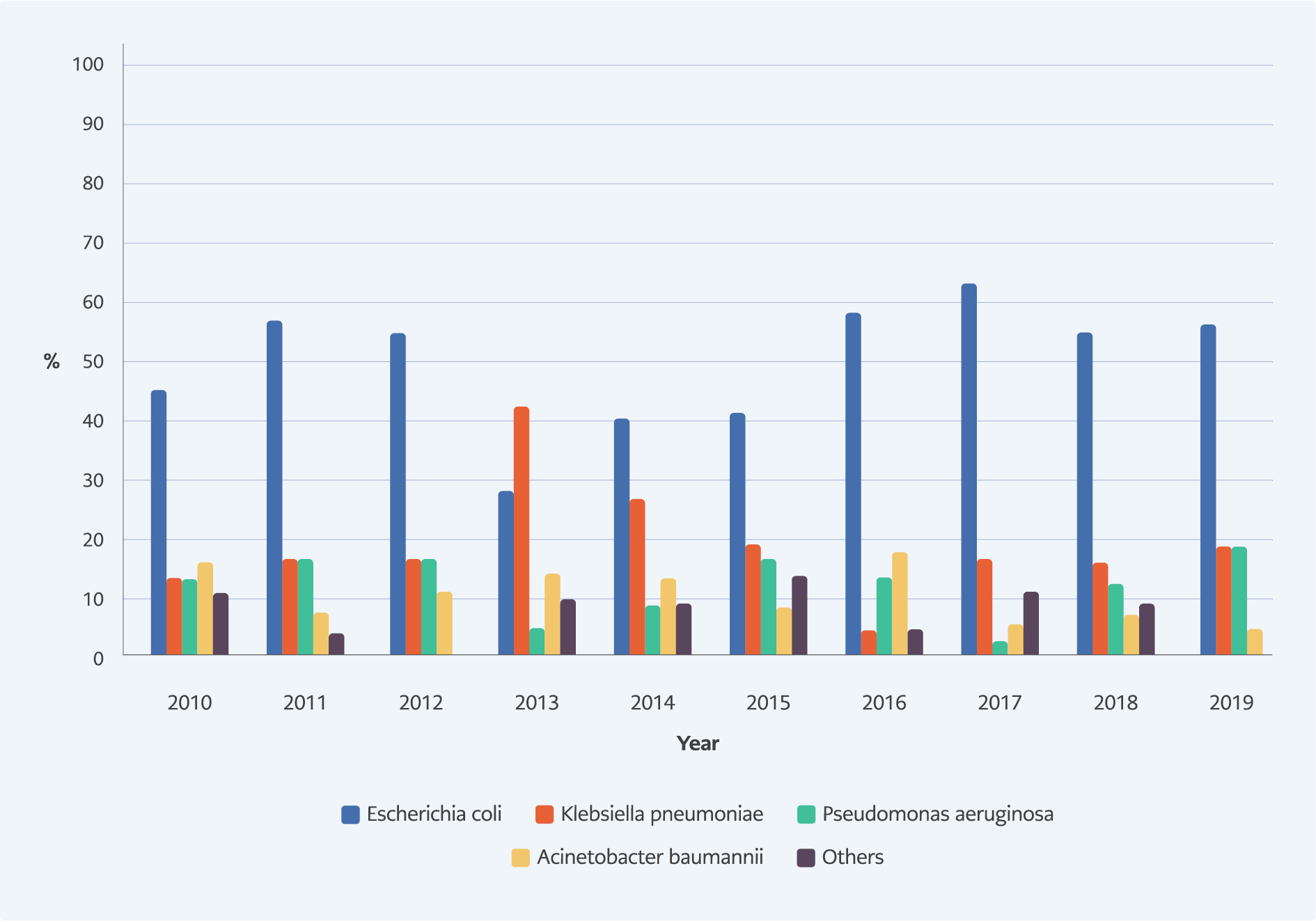
Figure 2. The changes in isolation of bacteria between 2010 and 2019.
An increasing AMR rate in GNB has been observed in our center over the years. While there was no significant change in ESBLs-producing E. coli and K. pneumoniae (p=0.32) and resistance to carbapenems in GNB (p=0.10), an increasing trend was observed in MDR bacteria (p=0.03) and CRE (p=0.02). The changes in isolation of bacteria and AMR rates over the years in patients with HMs were displayed in Figure 1-2, respectively.
Discussion
In this prospective study with neutropenic HMs patients, we identified factors associated with GNB and 30-day mortality; and we found higher overall, 7-day, 14-day and 30-day mortality rates in these patients.
In our study, the percentage of ESBLs-producing Enterobacterales was 44.6%; CRE were isolated in 33.3% and in 13.6% of the bacterial growths, ESBLs positivity and carbapenem resistance were present together. The recent data from World Health Organization indicated that Turkey is one of the countries with high AMR rates along with Greece, Italy and other Eastern European countries (13). This epidemiology may be related to the fact that current established empirical antibiotic regimens may not cover the resistant bacteria leading to worse clinical outcomes that may occur in patients with FN. Therefore, the choice of empirical treatment should be modified per local epidemiologic data and the individual risk factors for resistant GNB.
In the current study, bacteremic patients were more frequently exposed to antibiotics before the bacteremic episode. Except for cephalosporins, all other antibiotics were used significantly more in these patients. Prior antibiotic use was not detailed in most studies conducted, and it was stated as ‘antibiotic exposure’ as a general expression. Previous antibiotic exposure, especially broad-spectrum antibiotics, is a well-known risk factor for the development of both bacteremia and AMR (2, 6, 7, 11, 18). It has been found that recent teicoplanin/ vancomycin/ linezolide/ daptomycin exposure was also associated with the development of GNB like other antibiotics for GN infections. This has been demonstrated in other studies in which the use of antibiotics was similarly detailed (11, 20). Additionally, empirical antibiotics included more frequent colistin-containing regimens, the duration of antibiotic treatment was longer, antibiotic changes were more frequent, the use of aminoglycosides and colistin in targeted antibiotic regimens and nephrotoxicity were higher.
Studies demonstrated that AML and allogeneic HSCT, prior antibiotic exposure and ICU admission, prolonged duration of hospitalization and neutropenia were risk factors for ESBLs-producing Enterobacterales bacteremia (11, 17-21). Having a prior culture that grew MDR microorganisms and receiving glucocorticosteroids were independent risk factors for MDR microorganisms related bacteremia in several studies (11, 22-25). Our results were in accordance with the results of these studies regarding the factors associated with GNB.
Male gender was a factor associated with acquiring GNB in our study. The literature included mixed results in this respect (17, 21, 23, 26). In our study, all-cause mortality was 47.0% in cases of GNB, compared to non-bacteremic controls at 25.0%. Seven-day mortality was also higher in cases of GNB (18.2%). Both 14-day and 30-day mortalities were higher, 25.8% and 30.3%, in cases of GNB, compared to non-bacteremic controls 6.1% and 10.6%, respectively. In studies of assessing mortality in bacteremic patients with malignancies, overall and 30-day mortality rates ranged from 20% to 42% (6, 9, 18, 19, 24, 27). Bacteremia due to resistant GNB (6, 11, 17, 19), receiving inappropriate antimicrobial treatment (17, 18), prolonged duration of hospitalization (24), sepsis and related situations (28-30) were significant factors associated with 30-day mortality. The risk factors for mortality detected in our study were similar to previously published reports.
Although chemotherapy-induced neutropenia is a risk factor for both bacteremia and mortality (6, 8, 11, 17) in previous studies, chemotherapy was found to be associated with a decrease in mortality in our study (Table 5). This result was attributed to the improved chemotherapy regimens in recent years.
There are several limitations of our study. These include a single center with a limited number of study population, the short follow-up period despite being a prospective study and the low number of bacteremic patients. In addition, after June 2014, the hospital automation system was changed. This may have caused a loss of information in the retrospective period when AMR was evaluated. Lastly, all antimicrobial susceptibility results were interpreted according to the CLSI until 2017 and EUCAST guidelines thereafter. This has caused some changes in the AMR definitions (e.g.: MDR, XDR…) due to the MICs values in the guides. However, since the results were reported in line with the guidelines adopted by the hospital laboratory, we had also adapted to this change and made our definitions according to the new guideline.
In conclusion, our results identified several factors associated with GNB and mortality in a high-resistance setting. Applying these factors in a personalized decision-making analysis in febrile neutropenic patients may lead to a better management strategy.