Introduction
Coronavirus disease 2019 (COVID-19) is a potentially life-threatening disease caused by SARS-CoV-2. Clinical findings of COVID-19 are ranged from asymptomatic to severe pneumoniae, acute respiratory distress syndrome, multiorgan failure and death. A severe COVID-19 course is associated with a higher inflammatory state (cytokine storm) due to the excessive release of pro-inflammatory cytokines (1). Several cytokines, such as interleukin-1 (IL-1), tumor necrosis factor-alpha (TNF-alpha), and interleukin-6 (IL-6), are responsible for the development of cytokine storms in patients with COVID-19 (2). Several risk factors are associated with poor outcomes and high mortality in patients with COVID-19. Advanced age, male gender, and presence of comorbidities such as diabetes mellitus and hypertension are well-defined risk factors for severe COVID-19 course (3). Similarly, patients with COVID-19 accompanying cancer have been reported to have higher morbidity and mortality (4). On the other hand, predictive factors and treatment outcomes, including anti-cytokine treatment, are not well defined yet in patients with COVID-19 accompanying cancer.
Recent evidence showed that SARS-CoV-2 activates an intracellular multiprotein complex called ‘inflammasome’ after binding toll-like receptors. Inflammasomes are present in innate immune cells and have an essential role in the host’s defense against microorganisms, including viruses. The inflammasome senses the viral structures and activates caspase-1 for the cleavage of pro-IL-1β to produce active IL-1β. Anakinra, an IL-1 receptor antagonist, is commonly used to treat autoinflammatory diseases such as hereditary periodic fever syndromes, gout, and adult-onset still disease (5). Anakinra has also been proven effective in hyperinflammatory conditions such as macrophage activation syndrome, which is secondary to various diseases (6). In this study, we aimed to evaluate the outcomes of high-dose intravenous anakinra treatment in patients with severe and critically ill COVID-19 accompanying cancer.
Material and Methods
Patients and Data
This observational retrospective study is a secondary analysis of our previous study (7) carried out at a tertiary referral center between September 01, 2021, and February 01, 2022, in Turkey. All patients had positive polymerase chain reaction (PCR), typical computer tomography (CT) findings, and clinical signs and symptoms attributed to COVID-19. Patients with negative PCR results and inconsistent CT findings with COVID-19 were excluded from the study.
The study population was divided into two groups: patients receiving high-dose intravenous anakinra (anakinra group) and patients treated with standard of care (SoC) in the control group. The severity of COVID-19 disease was evaluated according to National Institute of Health (NIH) severity scale (8) and only severe (NIH score 3; patients with SpO2 <94% on room air at sea level, PaO2/FiO2 <300 mm Hg, a respiratory rate >30 breaths/min, or lung infiltrates >50%) and critically ill (NIH score 4; patients have acute respiratory distress syndrome, septic shock that may represent virus-induced distributive shock, cardiac dysfunction, an exaggerated inflammatory response, and exacerbation of underlying comorbidities, as well as requirement of high flow nasal oxygen therapy [HFNO] or invasive mechanical ventilation [IMV]) patients in the ward were included into the study.
Written consents were obtained from the patients and the Ethics Committee of Aksaray University approved the study on February 24, 2022, with decision number 2022/04-09.
Laboratory Evaluation
Laboratory values such as hemogram, liver enzymes, creatinine, procalcitonin, C-reactive protein (CRP), ferritin, D-dimer, lactate dehydrogenase (LDH) at admission, and the peak levels of CRP, ferritin, D-dimer and LDH levels were recorded. The inflammatory state of the patients was evaluated according to the COVID hyperinflammatory syndrome score (cHIS), and it was calculated according to a combination of neutrophil and lymphocyte counts at the admission and the peak levels of CRP, ferritin, D-dimer, and LDH during the follow-up (9).
Treatment Protocol and Outcome
All patients received background corticosteroid therapy with 80 mg/day methylprednisolone (or its equivalent) and enoxaparin 0.4 mg/day at the admission and on consecutive days (standard of care). In both groups, empirical antibiotics were used only in patients with higher baseline procalcitonin levels (procalcitonin≥1 pg/mL). Anakinra was started in patients who did not respond to steroid therapy for at least two days or concomitantly with steroids in patients with higher risk and critical illness at admission. The average starting dose of anakinra was 400 mg/day intravenously and increased gradually to a maximum of 1600 mg/day if necessary (10 mg/kg/day). Anakinra and steroid treatment were administered until the hyperinflammatory response of the patients disappeared. Anakinra dose adjustment was performed by the same rheumatologist (MB) according to daily clinical and laboratory findings. Severe infection was defined as the development of opportunistic infection, intravenous antibiotics, sepsis, or requirement of intensive care unit (ICU) admission or the development of death due to secondary infection.
Statistical Analysis
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 21.0 (IBM Corp., Armonk, NY, USA). In descriptive statistics, discrete and continuous numerical variables were expressed as mean, ± standard deviation, or median (minimum-maximum). Categorical variables were expressed as frequency and percentage. Cross-table statistics were used to compare categorical variables (Chi-square, Fisher’s exact test). Normally distributed parametric data were compared with Student’s t-test, and non-parametric data that did not meet normal distribution were compared with Mann-Whitney U and Kruskal-Wallis tests. Kaplan-Meier and log-rank methods were used for survival analysis. Multivariate analysis was performed by using logistic regression. The statistical significance was set as p<0.05.
Results
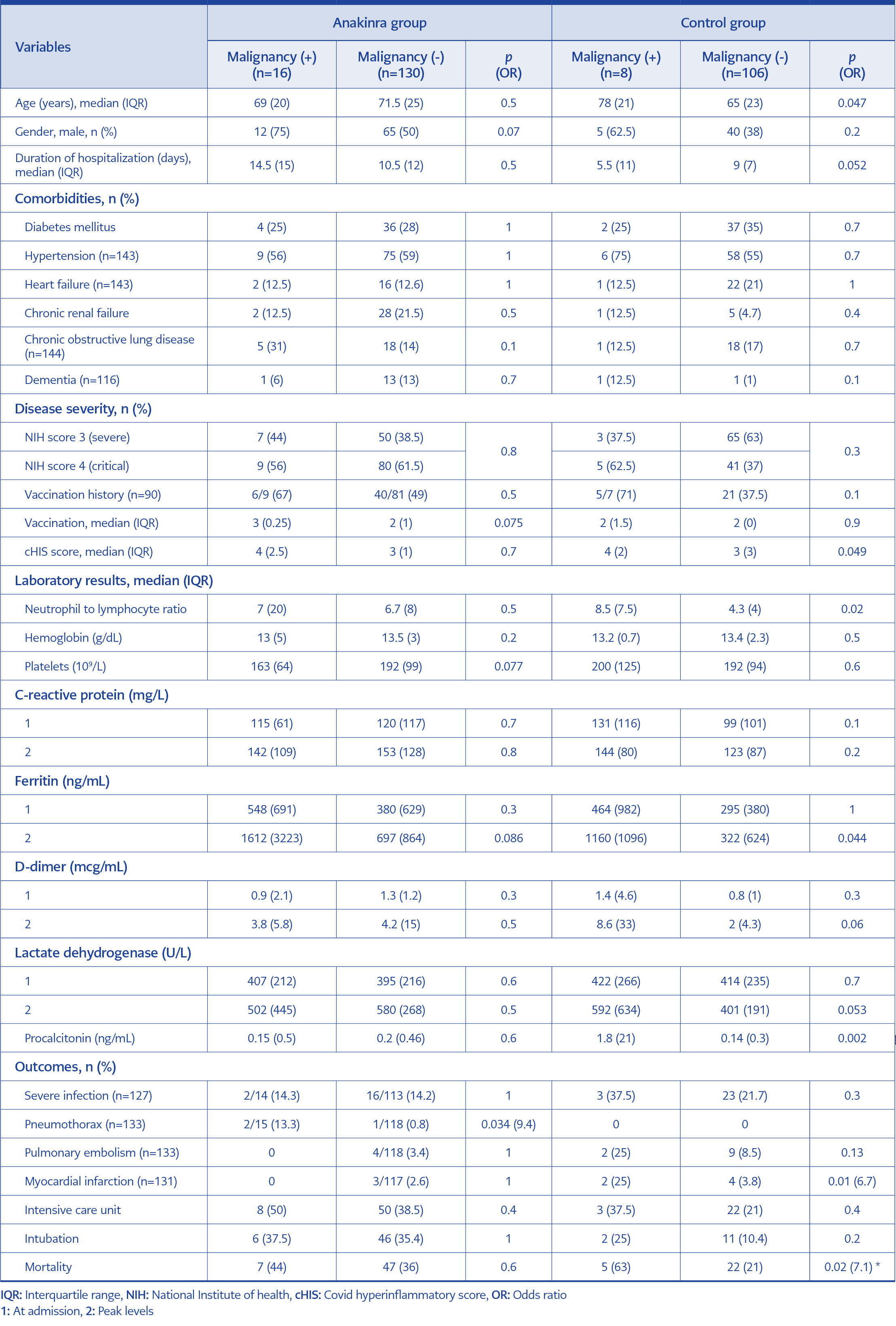
Table 1. Baseline characteristics and univariate analysis of patients with anakinra and control groups.
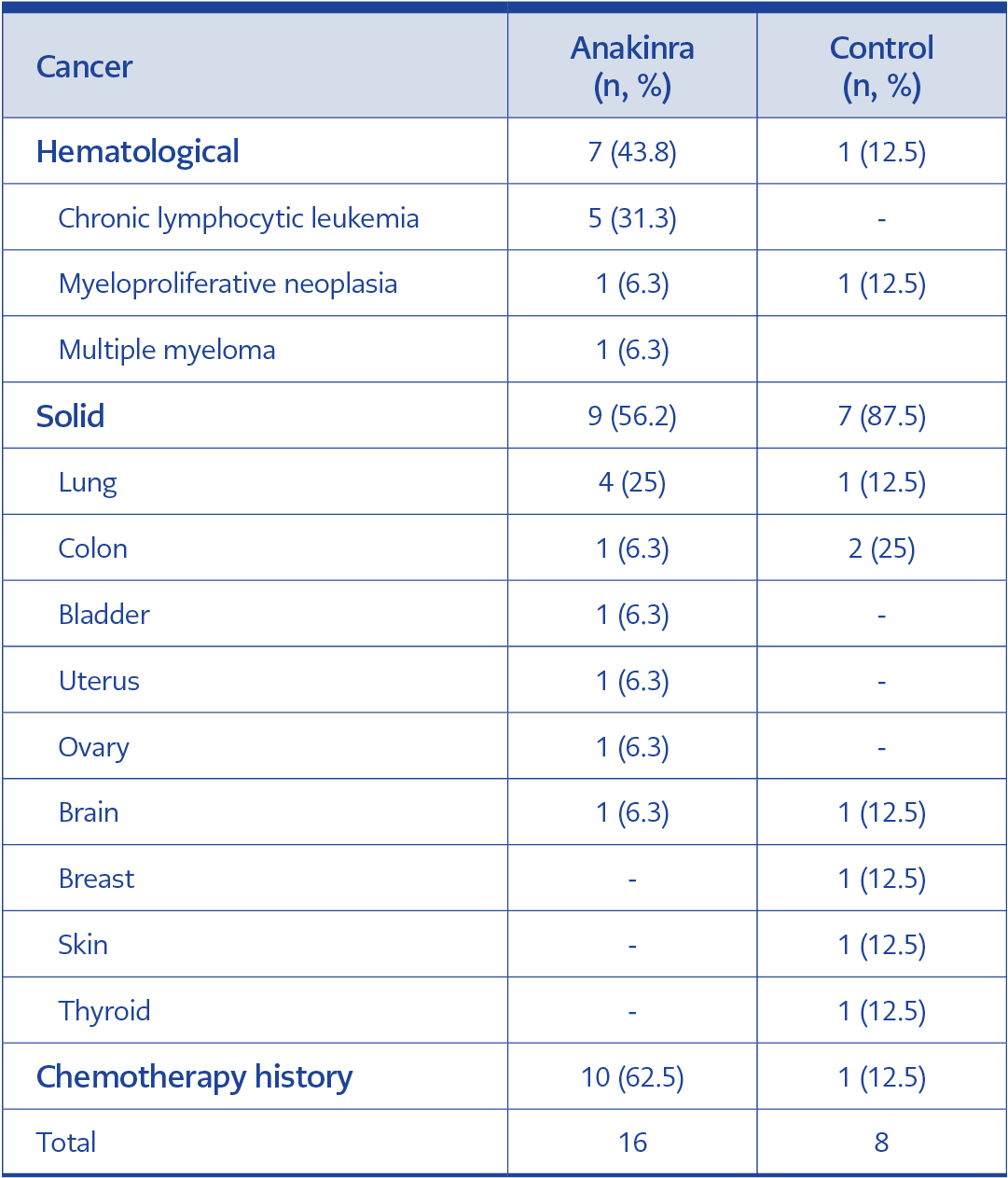
Table 2. Distribution of malignancies in patients with anakinra and control groups.
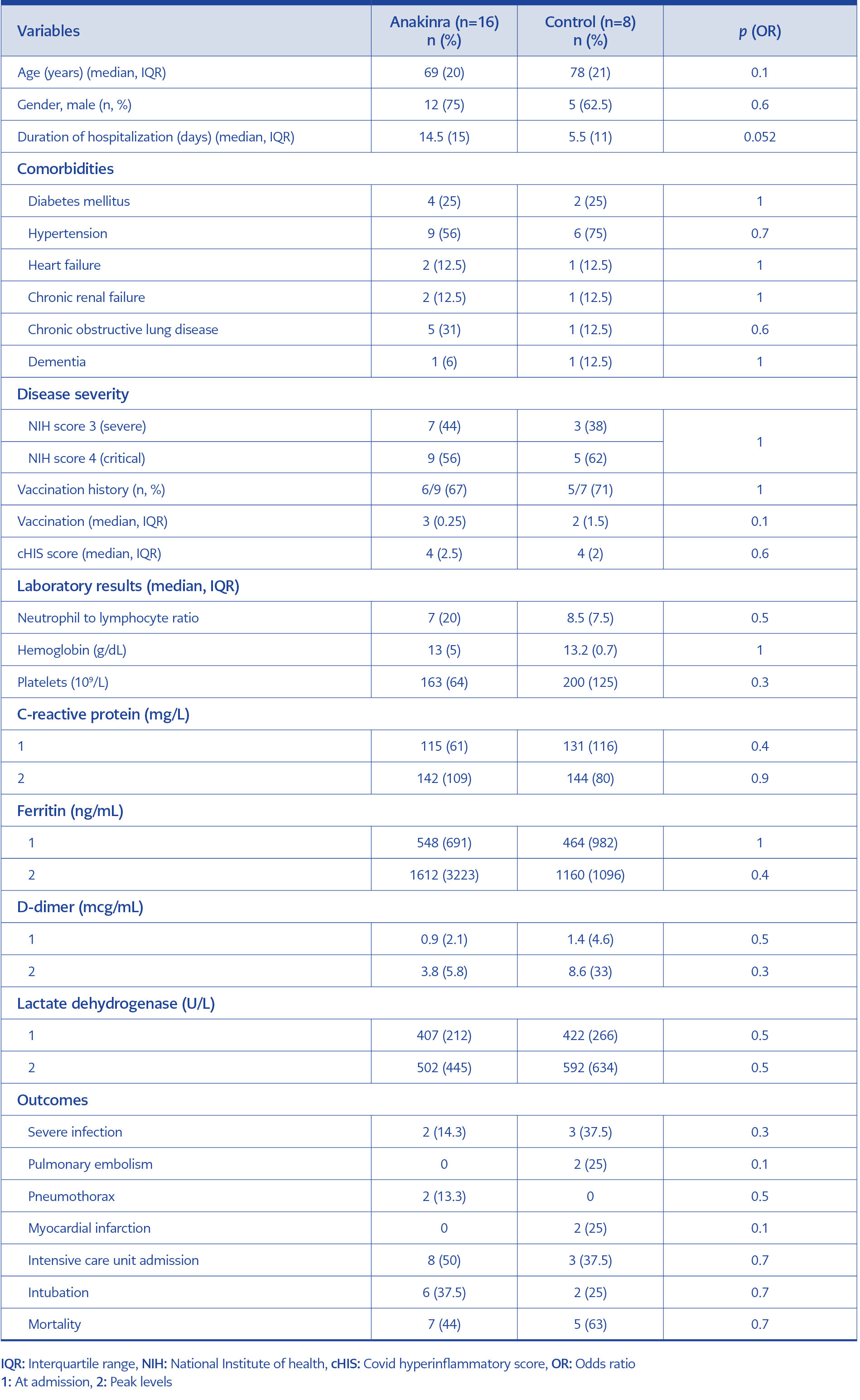
Table 3. Comparison of clinical and laboratory features of patients had malignancy between anakinra and control groups.
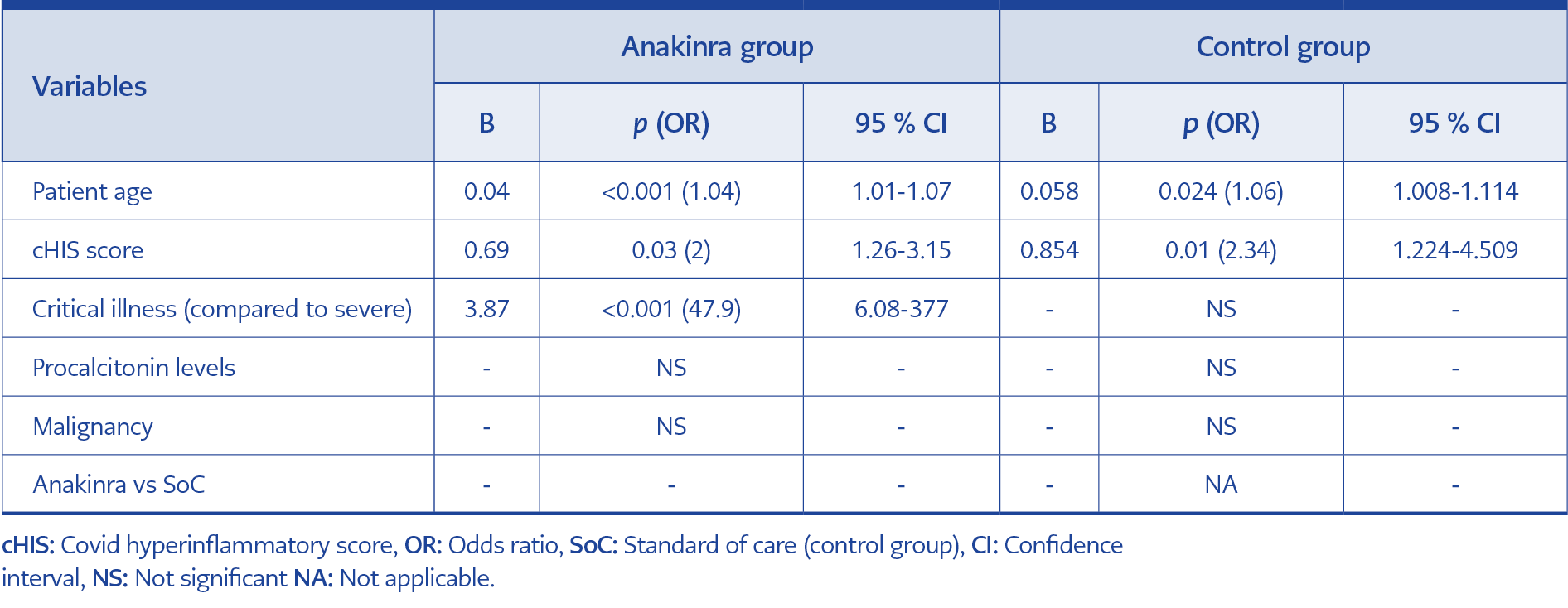
Table 4. Multivariate analysis of mortality-associated factors in patients with COVID-19.
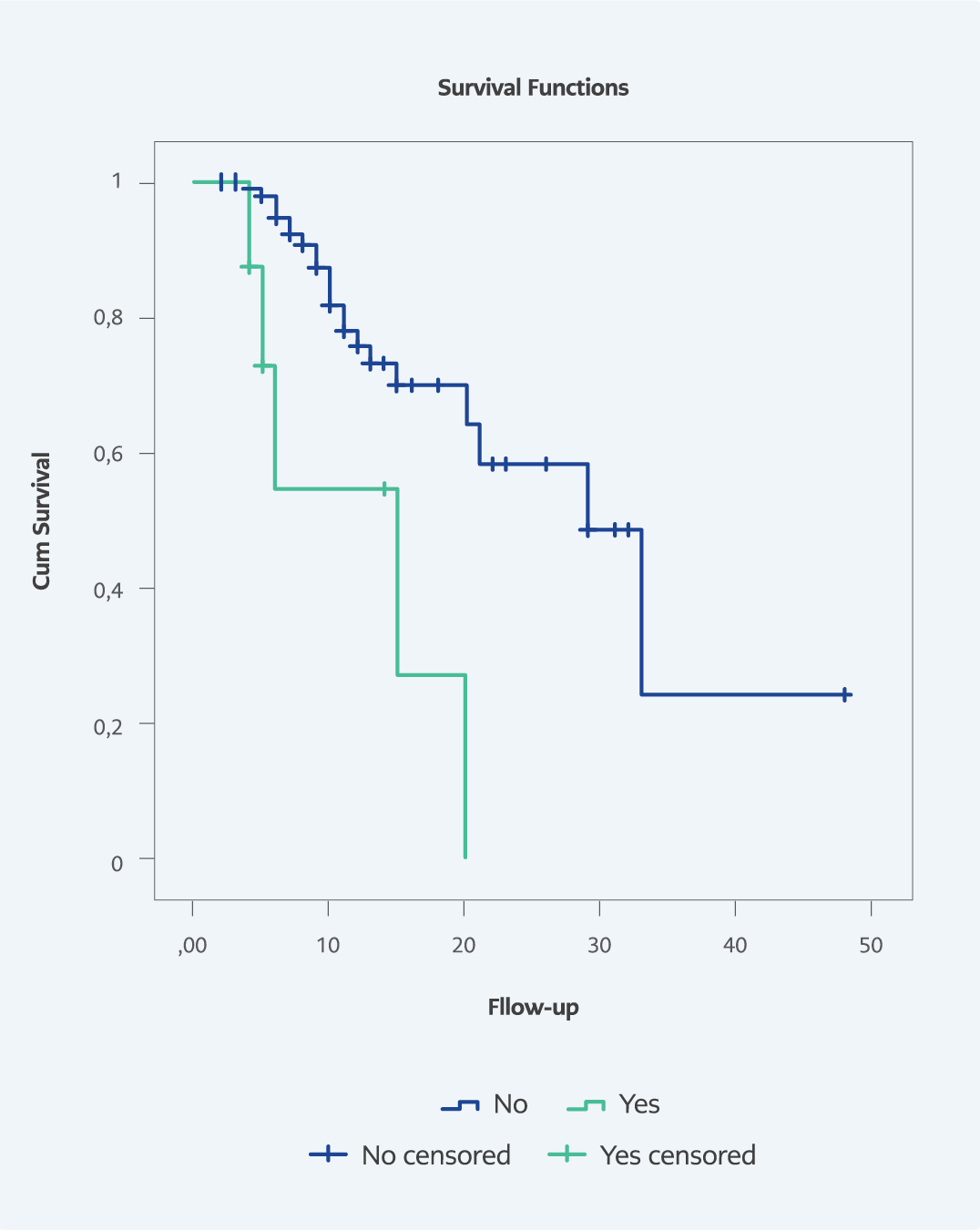
Figure 1. Comparison of mortality rate in patients with and without malignancy in the control group (Log-Rank: p=0.002).
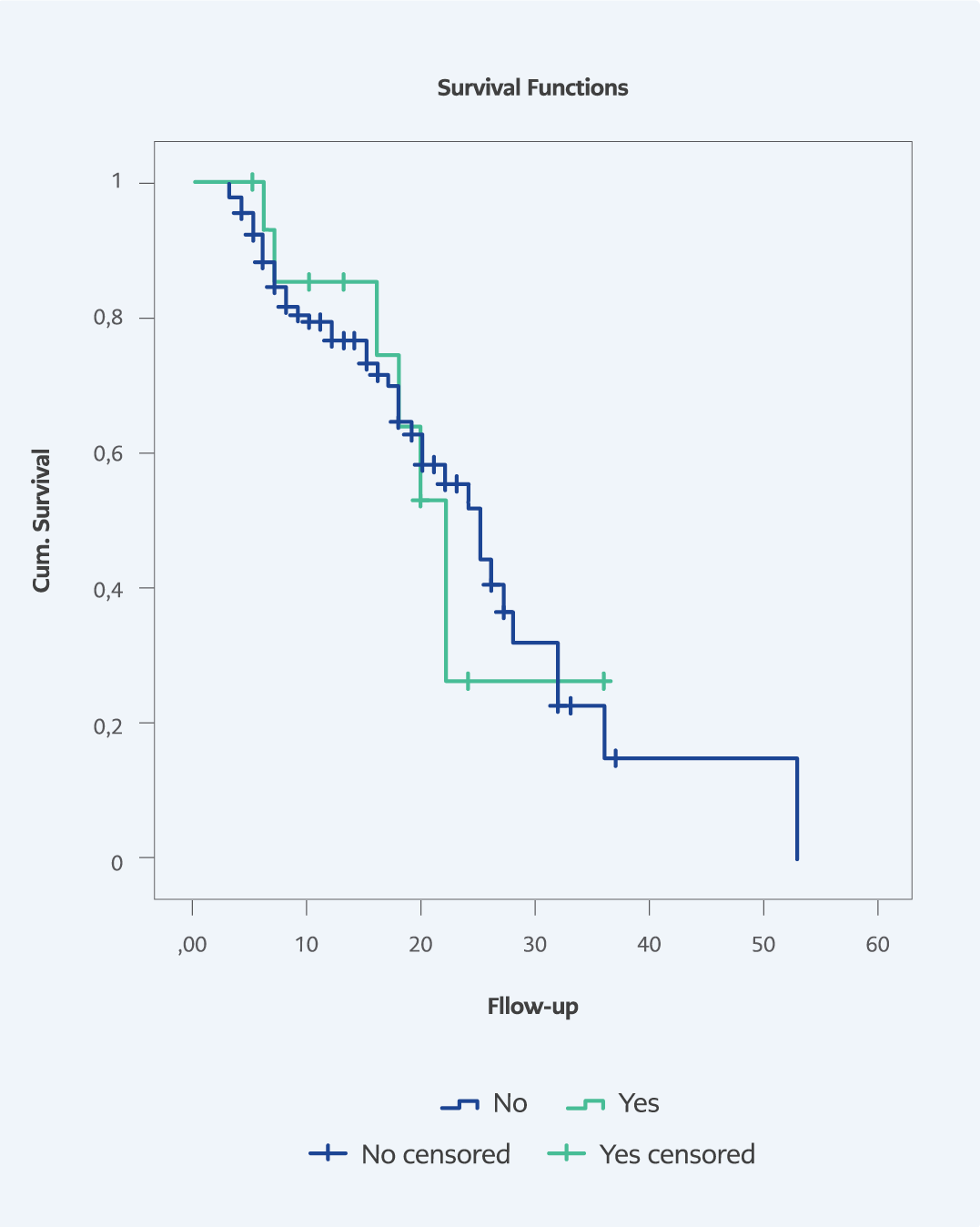
Figure 2. Comparison of mortality rate in patients with and without malignancy in the anakinra group (Log-Rank: p=0.9).
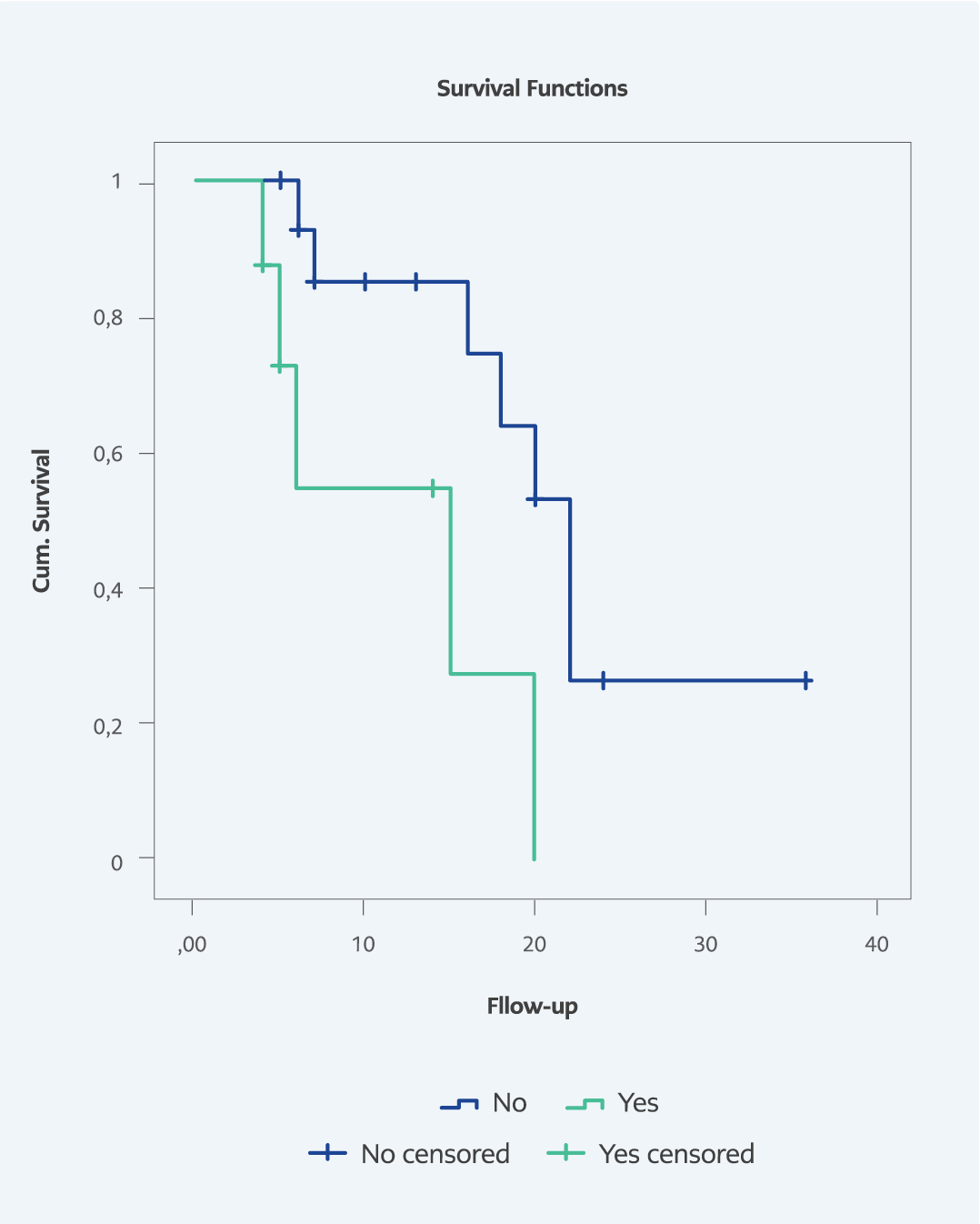
Figure 3. Comparison of survival rate in patients with malignancy between anakinra and control group (Log-Rank: p=0.013).
Data of 146 patients in anakinra and 114 patients in the control group were analyzed. Baseline clinical and laboratory findings of patients in the anakinra and the control group were described in Table 1, respectively. In the anakinra group, the median±interquartile range (IQR) patient age was 71 (25) years, and the duration of hospitalization was 11 (12) days, and in the control group, they were 65.5 (23) years and 9 (7.3) days. Anakinra and steroid therapies were applied for a median of 10 days (IQR=10, range; 2-36).
In the anakinra group and the control group, the rates of diabetes mellitus were 28% (n=40) and 34.2% (n=39), hypertension 58.7% (n=84) and 56% (n=64), heart failure 12.6% (n=18) and 20.2% (n=23), chronic kidney failure 20.5% (n=30) and 5.3% (n=6), chronic obstructive pulmonary disease 16% (n=23) and 16.7% (n=19), dementia 12.1% (n=14) and 1.8% (n=2), respectively. At admission, laboratory results revealed median (IQR) neutrophil to lymphocyte ratio (NLR) 6.75 (7.8) and 4.3 (4.4), CRP 119 (110) and 100 (100) mg/L, LDH 398 (206) U/L, ferritin 397 (206) and 414 (229) ng/mL, D-dimer 1.24 (1.2) and 0.84 (1) mcg/mL in the anakinra group and the control group, respectively. Peak levels of laboratory values were CRP 151 (122) and 126 (88) mg/L, LDH 566 (268) and 408 (237) U/L, ferritin 717 (980) and 378 (660) ng/mL, D-dimer 4.2 (13.3) and 2.24 (5) mcg/mL in the anakinra group and the control group, respectively.
Fifty-seven (39%) and 68 (59.6%) patients had severe, 89 (61%) and 46 (40.4%) had critical disease in anakinra and control group, respectively. Median (IQR) cHIS score was 3 (1) and 3 (3) in patients receiving anakinra and SoC, respectively. Overall, ICU admission was in 58 (39.7%) and 25 (22%), intubation was in 52 (35.6%), and 13 (11.4%) patients, 54 (37%) and 27 (23.7%) patients died in the anakinra group and the control group, respectively.
Malignancy frequency was 11% (n=16) in anakinra group and 7% (n=8) in the control group. The distribution of malignancies is shown in Table 2. Among the control group, the patients with malignancy significantly had higher patient age (p=0.047), baseline NLR levels (p=0.02), cHIS score (p=0.049), baseline procalcitonin (p=0.002), peak ferritin levels (p=0.044) as well as higher development of mortality (63 % [n=5] vs 21 % [n=22]; p=0.02, odds ratio [OR]=7.1) in univariate analysis. Although the number of male genders (p=0.07) and peak ferritin levels (p=0.086) tended to be higher, platelet levels (p=0.077) tended to be lower in patients with malignancy than those without in the anakinra group. While ICU admission (p=0.4), intubation (p=1), and mortality (p=0.6) did not differ between the patients with and without malignancy in patients receiving anakinra, development of pneumothorax was higher in patients who had malignancy (p=0.034; OR=9.4).
Clinical and laboratory values were similar between anakinra and control groups when comparing the patients with and without malignancy. ICU admission, intubation, and mortality also did not differ between the two groups (p=0.7, p=0.7, and p=0.7, respectively) (Table 3).
In multivariate analysis, advanced age and higher cHIS score were significantly associated with mortality in the anakinra group (p=0.002, OR=1.044, 95% confidence interval [CI]=1.016-1.073, and p<0.001, OR=2.3, 95% CI=1.5-3.4, respectively) and the control group (p=0.007, OR=1.04, 95% CI=1.01-1.07, and p=0.003, OR=2, 95% CI=1.26-3.15, respectively). Critical illness (compared to severe) (p<0.001, OR=64.9, 95% CI=8.3-505.2) was only significantly associated with mortality in the anakinra group (Table 4).
In survival analysis, a significantly lower survival rate was observed in patients with malignancy than those without in the control group (log-rank: p=0.002) (Figure 1) and patients with malignancy in the control group compared to anakinra (log-rank: p=0.013) (Figure 2). Still, it did not differ between patients with and without malignancy in the anakinra group (log-rank: p=0.9 (Figure 3).
Discussion
In COVID-19, mortality rates differ according to several variables, such as features of the study population (hospitalized vs. outpatient patients or ward vs. ICU), inflammatory burden, and disease severity of patients. Many studies have revealed higher mortality rates among severe and critical COVID-19 patients so far. Grasselli et al. found that overall mortality was 53.4% in their study with 3988 ICU patients (10). In another observational study with hospitalized COVID-19 patients, mortality was observed in 50.5% of severe and critical diseases according to the Brescia-COVID respiratory severity scale and 58% according to the CURB-65 scale, which was higher compared to our study (11). Our study population consisted of severe and critically ill patients, according to the NIH scale, for whom a higher risk of mortality was expected. There is also a close association between higher inflammatory response and mortality in patients with COVID-19 (12). The fact that the average higher cHIS score than originally described in the study also reflects a higher inflammatory burden in our study (9). Therefore, our study group had more severe disease and higher mortality risk at admission, which was expected to have a higher mortality rate compared to previous studies.
Beyond the demographic risk factors such as age and gender, some patients, such as patients who have cancer or are on immunosuppression, are at higher risk of mortality in COVID-19 (4).Miyashita et al. revealed significantly higher mortality risk (relative risk=5.01, 95% CI=1.55-16.2) among cancer patients <50 years in patients with COVID-19 (13). In the study by Tian et al., in addition to several traditional risk factors such as advanced age, elevated procalcitonin, ferritin, D-dimer, and IL-6 levels, the authors also reported a significant association between advanced tumor stage as well as elevated TNF-alpha levels and severe disease COVID-19 course among cancer patients (14). In our study, although procalcitonin levels were higher in patients with malignancy in SoC compared to those with anakinra group in univariate analysis, procalcitonin levels were not associated with higher mortality in multivariate analysis. Poor outcomes in cancer patients with COVID-19 may be associated with accompanying comorbidities, higher complication rates such as secondary infection, and higher disease severity due to the development of cytokine storms.In our study, although comorbidities did not differ among the two groups, higher patient age and higher inflammatory parameters (ferritin, CRP, D-dimer, cHIS score) reflecting cytokine storm in patients with malignancy than those without were observed in the control group.
Similarly, higher peak ferritin levels in patients with malignancy than those without malignancy in the anakinra group were consistent with the control group. On the other hand, there was no difference in severe infection and comorbidities but a higher inflammatory state in patients who had malignancy than those who did not, emphasizing the crucial role of cytokine storm in the development of mortality in patients with COVID-19 accompanying cancer. In a previous study from Turkey, the mortality rate did not differ between patients with and without malignancy who received anakinra; however, the study did not include a control group (15).
Recent evidence revealed that there is a link between the production of pro-inflammatory cytokines and the development or progression of some cancers. Several pro-inflammatory cytokines, such as IL-1β, IL-6, TNF, IL-8, and IL-17, were associated with advanced stages of breast, prostate, and colon cancer (16). Higher cytokine levels due to the lysis of cancer and stromal cells were also shown during chemotherapy and radiotherapy in patients with cancer (17). An emerging highly effective treatment, chimeric antigen receptor (CAR) T-cell therapy, was developed in patients with hematological malignancies (18). The development of cytokine release syndrome due to CAR T-cell therapy and its successful treatment with tocilizumab established the higher risk of hyperinflammation in cancer patients (19).
Furthermore, successful treatment with immune checkpoint inhibitors in several cancers also emphasized the crucial role of the immune system in the development or progression of cancer (20). In our study, higher hyperinflammatory state of patients with malignancy than those without malignancy both in the anakinra and control group was consistent with previous results. The development of cytokine storms was also associated with higher mortality in our study. Although the mortality rate did not differ between anakinra and SoC, possibly due to a small sample size (type 2 error) in univariate analysis, survival analysis revealed a lower mortality rate in patients with malignancy in the anakinra group than in SoC. Furthermore, our study also showed that treatment with anakinra reduces mortality due to the controlling hyperinflammatory response in patients with COVID-19 accompanying cancer. Further studies are needed to clarify the anti-cytokine treatment response, including anakinra, in patients with COVID-19 accompanying malignancy.
IL-1 is a crucial cytokine in the development of periodic fever syndrome, adult-onset still disease, and several hyperinflammatory conditions such as macrophage activation syndrome and hemophagocytic syndrome due to various immune-related disorders, infections, and malignancies (21). Furthermore, the safety and efficacy of IL-1 inhibitors such as anakinra were established in many studies in cytokine storms due to various diseases (22). Anakinra became one of the standard targeted treatments for the COVID-19-associated cytokine storm since the beginning of the pandemic (23). In a previous study, the survival rate was higher in patients receiving IL-1 inhibitors compared to IL-6 inhibitors. In this study, higher CRP levels at baseline and decreasing levels of LDH with treatment predicted higher IL-1 and IL-6 inhibitor response and reduced mortality.
Furthermore, differences in study dates (February and March 2020) between the former study and our study may have caused a difference in the mortality rate due to potentially different COVID-19 variants since the delta variant was not dominant into this period. Higher disease severity and poor outcomes with the delta variant compared to other variants were established in previous studies (24). Intravenous and high-dose anakinra is an emerging therapeutic option both in rheumatology and COVID-19. Intravenous anakinra enables higher and faster maximum plasma concentration compared to subcutaneous administration. Recently, there has been sufficient evidence of high-dose intravenous anakinra administration in hyperinflammatory syndromes (25, 26). High-dose intravenous anakinra treatment was safe and effective in a preliminary retrospective study from Italy and our previous study in patients with COVID-19 (7, 27). In another prospective controlled study (ESCAPE study) with critically ill COVID-19 patients, high-dose intravenous anakinra had a lower mortality rate than standard care as well as tocilizumab treatment (28).
Although data on the safety and efficacy of anakinra in cancer patients are limited due to the exclusion of cancer patients from prospective studies, recently, data on this issue has started to increase (6). No increase in the frequency of severe infection, as well as other complications such as myocardial infarction in the anakinra group compared to controls, indicate that high-dose intravenous anakinra is safe in patients with COVID-19 accompanying cancer. Daily dose adjustment of anakinra allows early intervention of the hyperinflammatory state, preventing unnecessary high dose administration according to daily clinical and laboratory parameters and withdrawing the drug in case of infection. The short half-life of anakinra may allow it to easily adjust daily doses in acute and critical diseases such as COVID-19-associated cytokine storms. This issue is an important advantage of anakinra over other anti-cytokine treatments such as tocilizumab.
This study has some limitations. The retrospective design of the study is the main limitation. The relatively lower frequency of cancer patients among COVID-19 is another limitation. Additionally, the lower frequency of patients receiving chemotherapy did not allow for comparison. Other limitations include higher patient age (not statistically significant) and procalcitonin levels at admission between anakinra and SoC groups in patients with malignancy. On the other hand, the controlled design of the study and the fact that the study was conducted in a single center ensures homogeneity in terms of patient population and treatment decisions that a single physician made.
In our study, mortality developed in a third of anakinra receiving severe and critically ill COVID-19 patients. Patients with malignancy had higher hyperinflammatory responses than those without malignancy both in the control and anakinra groups. Mortality was higher in patients with malignancy compared to those without malignancy in the control group but not in the anakinra group; it was also higher in patients receiving SoC compared to anakinra. Our study indicates that cytokine storm is the leading cause of mortality in patients with COVID-19 accompanying cancer. Intravenous high-dose anakinra treatment is safe and effective in cancer patients with COVID-19-associated cytokine storm.