Introduction
It would be apt to refer to the 20th century as a period of forgetting or not remembering in terms of the history of medicine in general and history of epidemics in particular. A historian of medicine, Frank Snowden, refers to this state as historical amnesia (1). With the sense of fear and danger that COVID-19 pandemic has instilled in people, the curiosity regarding the past epidemics or pandemics and their history has increased accordingly. As Curtis and Van Besouw state, “As COVID-19 continues to cause further suffering across the world, historians have suddenly been in demand. Opinion pieces are piling up day after day, and every historian — regardless of whether they work on epidemic disease or not — has a view” (2).
The most frequently posed questions to the historians these days are similar and require a sort of historical prescription. Some common questions that arise are as follows:
- What happened in the past epidemics or pandemics?
- What kinds of reactions were given then?
- What lessons can be drawn?
Although there have been efforts to compare COVID-19 with past pandemics and draw lessons accordingly, the experts have warned us, especially about the limits of drawing historical analogies, because they constrain our ability to grasp the complex place-and-time-specific variables. When the present is viewed through the lens of former disease outbreaks, we typically focus on similitudes, and sometimes analogies create blind spots (3).
This article does not aim to compare COVID-19 with cholera or provide ready-made answers to the abovementioned questions. Instead, it aims to recall a forgotten history of epidemics and rethink this history in the context of the current pandemic. To this end, I will try to present some of the experiences and findings of Luigi Mongeri, the former quarantine physician who witnessed many epidemics during the 19th century, and later became the most renowned psychiatrist of Istanbul. I believe his experiences and insights will contribute to our current efforts in rethinking the pandemic that we have been experiencing. Therefore, the article will focus on certain social, political, and psychological behavioural patterns rather than trying to establish a relationship of similarities or differences between the cholera epidemic that erupted in the middle of the 19th century and the current pandemic.
At the outset, I would like to briefly explain why I have chosen Mongeri for this article’s purposes. I will then summarise the historical background of the period. If we are to look at the history of epidemics or pandemics in an attempt to grasp better and understand the current pandemic, many elements from different epidemics belonging to different centuries and geographies would certainly help us. In such a study, we could sometimes also run into texts written about similar issues in different periods, and we might definitely learn a lot from them. Studying the writings of people who personally witnessed an epidemic could also be of interest to us.
If the writer in question is also a physician who combats the epidemic, then his writings not only focus on the medical discussion of the epidemic, but also draw attention to the political, economic, and social aspects of the epidemic by offering insights into the mentality of the people of the period. In this case, the individual’s writings become even more valuable. All of these distinctive qualities characterise Mongeri’s life and writings. The reason why I have chosen to focus on only one of the many texts that Mongeri wrote about the cholera outbreak is that this text has all characteristics mentioned above. Also, Mongeri’s body of work regarding epidemics is quite expansive, extending well beyond what we are trying to establish with this article.
Historical Background: Cholera Epidemic in the Nineteenth Century
In many ways, cholera was he premier disease of the 19th century, and was a fundamental component in the development of modern public health. Until the early 19th century, cholera was endemic to the Ganges Delta in Bengal, India. The first cholera pandemic occurred in the Bengal region of India in 1817. The disease spread from India to Southeast Asia, the Middle East, Europe, and Eastern Africa (4). Cholera first reached Europe in 1830, causing mass mortality, panic, and unrest (5). During the first wave of the outbreak, the strategies adopted by health officials were essentially those that had been used against the plague. New lazarettos were opened, especially in European ports, and quarantine measures were applied to prevent miasmic transmission between places.
Cholera led to heavy demographic, political, social, psychological, and economic losses in the Ottoman Empire (6). At the same time, with the outbreak of cholera, modern quarantine practices and public health measures began to be formed or shaped in the Ottoman Empire. The first temporary quarantine was implemented in the capital in 1831 when the cholera pandemic spread to Istanbul (7). Following this first temporary quarantine that ensured the quarantining of the ships that came from the direction of Black Sea, the quarantine that was implemented in Çanakkale in 1835 required keeping a close watch on the ships that would depart in the direction of Marmara and Istanbul (8). The transition to modern quarantine implementation in the Ottoman Empire was by no means easy. There were varied and severe reactions from the bureaucracy and the public (9). The quarantine method was formally accepted in 1838, and Quarantine Organization was established, and new lazarettos were gradually organised especially in port cities (8,9). In the Ottoman Empire, which encompassed a vast territory, cholera broke out in different cities between 1848-49. As it did in many countries, cholera replaced the plague to become the greatest fear of both the people and administrators in the upcoming years.
A great discussion continued throughout the major part of the 19th century with regard to the etiology of cholera. Basically, there were two theories, namely contagionism and anti-contagionism. Anti-contagion theory, also known as Miasma Theory, claimed that the source of diseases was bad air and that diseases were transmitted by inhaling and not from person to person (5). Contagion theory, named as Germ Theory after the discovery of microorganisms, claimed that diseases were transmitted from person to person, and germs were the source of epidemics and disease. The period of cholera epidemics in the 19th century witnessed this debate between contagionists and anti-contagionists (10), and a transitional period to germ theory began in the late 1850s with the work of Louis Pasteur, which was extended by Robert Koch in the 1880s. During the cholera pandemics (1848-49), most physicians were anti-contagionists who refused to believe that invisible organisms could spread disease. Luigi Mongeri worked as a sanitary physician in the 1840s and wrote about cholera in the 1850s within this historical context.
An Italian Physician in the Ottoman Empire at the time of cholera
Luigi [Louis] Mongeri was born in Milan in 1815. He graduated from the renowned School of Medicine in Pavia. When he was still a student, he conducted research on the etiology of cholera in the general hospital in Milan. As a young medical student, Mongeri wrote a review addressing the contagiousness of cholera on the basis of his observations at this department (11). In retrospect, we can say that this was his first test with respect to infectious diseases. Even though the review was outside the purview of the dominant paradigm, it challenged that paradigm with the courage of youth, and was exceptionally well received by his supervisor.
Mongeri was offered a position at the school of medicine, but he refused for political reasons. As a young student, he also participated in various revolutionary groups that opposed the Austrian occupation of Italy. Mongeri, whose country was occupied by foreign forces at the time, shared all the convictions and principles of the entire Italian youth with fervour and always considered himself in danger in political terms. He came to Istanbul on May 24, 1839, and, almost as soon as he arrived, he was employed as a physician in the Ottoman Army, which was then fighting the Egyptian forces in the Battle of Nizib. He returned to Istanbul and was employed in the International Quarantine Organization. Mongeri worked in Sinop and organised the quarantine department there. He was then appointed as a sanitary physician to the island of Crete, and served at this post until 1849 (12).
During his time in Crete, Mongeri was quite interested in the cholera epidemic, which at the time was the most important health problem on the island. Later on, he published his cholera experiences in Crete in the form of several articles, which were collected in a book in the following years (12, 13). He became notorious for his introduction of the strict isolation of patients. These drastic measures disturbed the Supreme Council of Health in Istanbul, and consequently, the government dismissed him in 1849 (11, 12). Mongeri refused to be assigned to someplace else. Even though he was later asked to return to his old duty, it was too little too late.
During the approximately eight years that he worked on the island of Crete, he devoted nearly all of his working hours to prevent a cholera outbreak there. He intended to ensure that in case the outbreak could not be prevented, at least it did not spread across the island, and it could be contained as quickly as possible. He shared his experiences and views on outbreaks during this period with the medical fraternity through a series of articles following his return to Istanbul.
Mongeri returned to Istanbul in 1851 and was assigned to Suleymaniye Lunatic Asylum in 1856 as the Chief Physician (14). This period coincided with the Crimean War (1853-56), marking the Ottoman Empire’s fight against Russia with the help of the United Kingdom, France, and Piedmont. The European physicians that were in Istanbul due to the war established a society called Société Impériale de Médecine. A year after its inception, the journal of this society called Gazette Médicale d’Orient was published (15).
Gazette Médicale d’Orient was the most long-standing medical journal, which was published in Turkey during the Ottoman Empire. At the time, the language of medicine across the world was French. The language of education of the School of Medicine –Mekteb-i Tıbbiye– that was opened in Istanbul in 1827 was French as well (16). In brief, Mongeri wrote about his ordeal with epidemics in Gazette Médicale d’Orient, published by the medical society, with which he was associated as one of the founders. In the 8th issue of the journal published in November 1857, his first article on the cholera epidemic titled De la nature contagieuse du choléra et des devoirs des médecins sanitaires (17) was published.
Sacrifice and Courage vis-á-vis Ignorance and Lethargy
In the introductory part of the article titled De la nature contagieuse du choléra et des devoirs des médecins sanitaires, Mongeri states that physicians have a serious task concerning people’s health. However, a physician’s real task emerges when public health is at risk. During an epidemic, physicians have to work in a field filled with difficulties and obstacles.
“The role of the physician that has great seriousness when it concerns only the health of the individual becomes even greater and takes on the quality of a sacred duty when the physician turns into a guardian responsible for the health of the public. A vast field now opens up before him, a field that bristles with difficulties and obstacles of all kinds. Is it about putting an end to the pervasive march of an epidemic? On the one hand, there is ignorance and lethargy resisting all measures that could effectively ward off disaster, and on the other hand, there are prejudices and habits that can preach futile practices, inspired by senseless fear. These are immediately in struggle with each other. By force of energy and perseverance, as soon as he succeeds in erecting a dike against the enemy and enclosing it within narrow boundaries, the blindness of the populations concerned or the embarrassing ignorance of the administration often destroys in an instant the result obtained painfully.”
“Have medical doctors always been aware of their sacred mission? Of course, self-sacrifice and courage have never failed them, and this is one of the glories of our profession, but it must be admitted that they sometimes lack intelligence and knowledge. The history of the plagues, which devastated Europe and the whole world, is there to attest that the introduction and the progress of these plagues have been facilitated by the insufficiency rather than by the incomplete execution of the measures against them” (17).
On the one hand, there are sacrifice and courage, and on the other hand there are ignorance and lethargy. These fundamental findings of Mongeri have been frequently voiced during the pandemic that we have been experiencing. Mongeri actually reached that conclusion by looking at the epidemics of the past. While talking about these previous epidemics, the first thing that comes to mind is usually the plague epidemic that lasted for centuries. Cholera first broke out at the beginning of the 19th century and then spread across the world by leading to a more serious pandemic starting from the 1830s. Therefore, it is not surprising that Mongeri draws a comparison between cholera and plague epidemics in terms of combatting them. We are also trying to find some parallels between the 21st century’s greatest pandemic, COVID-19, and the 20th century’s most severe pandemic, Spanish Flu, in terms of the struggle against them. This does not imply that history repeats itself. History does not repeat itself; however, the behavioural patterns of people, communities, and societies as a species might repeat themselves.
“The conflicts among schools, the mentality of the system, bad faith, and perhaps, even though it pains us to say it, a cowardly consideration for the self-seeking governments have prevented us from recognising the contagious nature of the plague, and in turn have led to its spreading and development.”
“Even nowadays, despite a dearly acquired experience, do we not see sterile theorists, despite the eloquent demonstration of the facts, spending dialectical force and subtleties to assign to the plague, in the name of a hypothetic science, a general cause? The facts say contagion, they respond epidemic influence; it used to be about the plague, now it’s about cholera” (17).
While stating that physicians made personal sacrifices and showed courage fighting against the epidemics, he emphasises that his colleagues sometimes lacked intellect and scientific knowledge. He was not wrong to say that. Among physicians, it was not very easy to accept that plague was an infectious disease. In addition, given the stereotyped thoughts of the period, the tendency of not questioning the mentality of the administrations, and even worse, the “cowardly consideration” towards the governments, which pursued their own interests rather than the society’s interests, Mongeri was right to maintain that the physicians themselves might lead to the spreading of the epidemics.
“To prove the contagious nature of a disease, we must first go back to its origin and then follow it through its cause and effect relationship. In Europe, everything is opposed to this kind of research. First of all, the means of communication are so rapid and so numerous, and the social gatherings are so tight and tangled, that the investigation easily loses track of the disease and manages to justify the idea that it is not contagious.”
“Constantinople and the other major maritime cities of the Ottoman Empire, are in the same condition as the cities of Western Europe in terms of speed of communication. It is difficult to go back to the origin of the disease and follow its traces. This difficulty is not found in the cities of the interior or in the islands of Ottoman Archipelago, and if the Health Council of the Empire had been able or wanted to employ the same instruments against cholera that it had employed against the plague, it would have been equally successful in its endeavours” (17).
The real obstacle for somehow not being able to put an end to the epidemics is of course not the physicians themselves, but, on the contrary, the people who govern an entire society, including the physicians, the governments, and even the people who affect their decisions, the interest groups so to speak.
“Added to this natural difficulty of research are the obstacles created by commercial greed that does not support any measure, even of public utility that could hinder its operations. Modern society is primarily concerned with facilitating acquisition. Its currency is the English currency: time is money. The wonderful discoveries that have erased distances enable the products and wealth to be exchanged and circulated with the rapidity of lightning, but the disease itself also follows the same route. To try to stop it is to attack the most powerful interests, confront the deepest passion of the time head on” (17).
As Ackerknecht argued, contagionism was not merely a theoretical or even a medical problem, it was a discussion about quarantines and politics:
“Contagionism had found its material expression in the quarantines and their bureaucracy and the whole discussion was thus never a discussion on contagion alone, but always on contagion and quarantines. To the rapidly growing class of merchants and industrialists, Quarantines meant a source of losses, a limitation to expansion, a weapon of bureaucratic control that it was no longer willing to tolerate. And this class was quite naturally with its press and deputies, its material, moral, and political resources behind those who showed that the scientific foundations of quarantine were naught, and who anyhow were usually sons of this class.
Contagionism would, through its associations with the old bureaucratic powers, be suspect to all liberals, trying to reduce state interference to a minimum. The anti-contagionists usually emphasised readily this popular aspect of the problem. They wrote long and detailed dissertations of exactly how many millions of pounds, francs, or dollars were lost yearly through the contagionist error” (10).
Mongeri states that as soon as cholera emerged, it divided the scholars into two camps called ‘contagionist’ and ‘anti-contagionist’:
“As soon as it was discovered, the cholera divided the scientists into two camps; for some it is due to particular atmospheric conditions, indeterminate, occurring at certain times, in certain places; others denying any atmospheric influence, believe that the disease is transmitted from person to person or objects to person in any climate, in any locality, in any season. You know, gentlemen, the disease and the discussions it has raised, you know also, that for some time the contagionist camp has grown a lot.
Among the new conversions, we will particularly mention that of Doctor Michel Lévy, one of the European medical celebrities, who, in his mission in the East during the war, was able to observe more than once the mode of origin and transmission of cholera: I have formally recognised and proclaimed its contagious nature and the measures that were adopted in consequence for the health of the French army and the science of the results that you all could appreciate” (17).
Psychological and political reactions to epidemics
Epidemics or pandemics are also a psychological phenomenon, and there were also psychological and societal reactions to them in the time of Mongeri. He observed that quarantine measures and sanitary rules are violated during the epidemics:
“Strict compliance with sanitary rules is often violated in Lazarettos. How much more difficult it will be in a country accessible from all sides, and it will become impossible if the essential element — the assistance of the inhabitants — were to fail. This element cannot be obtained by force or cannot be preserved by violence; it is the result of trust in authority, belief in the utility of sanitary rules, and respect for those who enforce them, and I thought I had to use it for general health.”
“The plague for example. The ridiculous incredulity that greets it at its beginning, the contempt of all preventive measures, and later, when the plague has been revealed, the dread, the loss of any presence of mind, and the adoption, in despair, of means least in harmony with reason and science, aren’t these constant facts? This annoying habit of being deaf to the lessons of experience, of beginning to deny through ignorance, which one ends up distorting and exaggerating under the influence of fear, is so peculiar to human race.”
“This same stubbornness to reject the truth, this shameful deception of the words used to sober it up, these belated concessions, torn away by the intensity of the peril, have we not seen them recur in connection with cholera? (17).
Given Mongeri’s place of duty, he had, without a doubt, a serious advantage of preventing the spread of the epidemic due to the fact that the entrance and exit points to the island were numbered. There were not many alternatives, and it was thereby easier to control the entrances. The residents of the island were also quite experienced on this subject because of recurrent plague and then cholera epidemics. For example, Mongeri revealed the case of bubonic plague in a ship coming from Egypt in 1842 and protected the island of Crete from the infestation of the plague by taking quarantine measures.
“This conviction was all the more profound among the inhabitants of the island of Crete, who appreciated the benefits of the quarantine institutions. Since their establishment in 1830, their island, which was threatened at eight different times with an invasion of the plague, had been preserved as many times, and they had seen that the disease was suppressed in the Lazaret. They had become such outraged contagionists that at the slightest epidemic, they demanded the application of sanitary measures. This is what happened in 1848, when cholera was rampant in the provinces of the Empire. Yielding to their prayers, I then adopted prophylactic measures, which, however, were disapproved and suppressed by the Intendance Générale. A year later, cholera broke out on the island and the sudden greatness of the danger was such that, out of conscience, and to avoid public blame, I believed I had to disobey the higher orders: I adopted the principle that in the sciences of observation and experience, a fact has more weight than any scientific authority, and I did not hesitate, in order to stop and destroy the scourge, to resort to the very means which the administration had condemned as useless and inapplicable” (17).
It is understood that Mongeri had no hope from Istanbul. Istanbul had got rid of the cholera disease, as was officially proclaimed on October 18, 1848, but in the countryside, the epidemic was seen occasionally until January 1849. In the first week of October, the Quarantine Council abolished the quarantine for all ships except those that had cholera on board. Right after this, the Quarantine Council claimed that since no more cases appeared in the city, the cholera epidemic in Istanbul had ended and that clean patents would be given to ships and passengers leaving the port. (18).
According to the Ottoman Empire’s official numbers, the total number of lives lost in the outbreak was 4,292. The cholera epidemic of 1847-48 was named as İllet-i Müthişe, which means “horrible disease”. Just when it was declared that the epidemic was finally over, Mongeri received the news that there was a cholera case in the village of Gaidouropoli in January 1849. He immediately went to visit the patient and began to investigate the place of its origin. After a short while, he was able to find its cause. A man whose daughter had passed away due to cholera a few days ago came to Crete by way of a ship from Kusadasi. He embarked on the ship with the pain of losing his daughter, and he hastily took her belongings with him. He got off the ship with a suitcase filled with underwear soiled with feces carrying cholera. When he arrived in the village of Gaidouropoli, he gave them to a washerwoman. At first, Mongeri identified and visited the people who were in doubtful contact with the infected person, who exhibited cholera symptoms through filiation. He then cut off the village’s contact with the other villages of the region and implemented strict quarantine measures (17).
Even though the orders coming from the centre told him to do the opposite, Mongeri persevered. He isolated cholera in a narrow area with strict quarantine measures, and the epidemic ended without spreading. In the meantime, his duty there was ended.
I have tried to summarize Mongeri’s first article on cholera. At the end of this article, he makes the following wish:
Mapping of the Cholera and the Cholera Outbreak in the Asylum
Considering the period, let’s look at the rest of the story by keeping in mind the existence of a highly-charged political relationship between Crete and Istanbul not only with regard to the management of the epidemic but also in general.
Mongeri departed from Crete together with the Governor of Crete, Mustafa Naili Pasha, and came to Istanbul in 1850. In 1851, he was assigned with the treatment of Sultan Abdulmecid’s sister Adile Sultan. In 1856, he became the Chief Physician in Suleymaniye Asylum. He set to work in order to reform this institution, which was in a miserable state and quite neglected (12, 14). His reforms and implementations, were to a certain extent, able to change the way society and bureaucracy perceived madness and asylums. He carried on his persistent studies that aimed to make psychiatry a field of medicine and science till his death (12).
As he did in the cholera epidemic, he examined the etiology and the course of mental illnesses and wrote down many articles and books on the subject. Of course, he did not entirely move away from the subject of epidemics. On the contrary, during the years he ran the asylum, his biggest fear was the eruption of an epidemic within the asylum. When a cholera epidemic broke out in Istanbul again in 1865, he worked actively. According to official statistics, 11 000 people died, but more reliable sources indicate that the real death count was around 20 000 (18).
Mongeri, who was appointed to the commission that was formed for handling the disease control measures, wrote a book about his observations and opinions concerning the epidemic. He also drew a map of the epidemic around the Bosphorus and its surrounding area (13).
In 1871, Mongeri witnessed another cholera epidemic, which resulted in the death of 3,000 people. And towards the end of 1873, his fears came true. A gastroenteric disease spread amid the patients of the asylum. Symptoms, such as vomiting, diarrhoea, low fever, pain, and cyanosis, accompanied this disease. According to Mongeri, this disease did not exhibit the characteristic symptoms of cholera (12, 14). However, Mongeri used this epidemic as an appropriate excuse to evacuate this quite dilapidated old asylum and move to a different place:
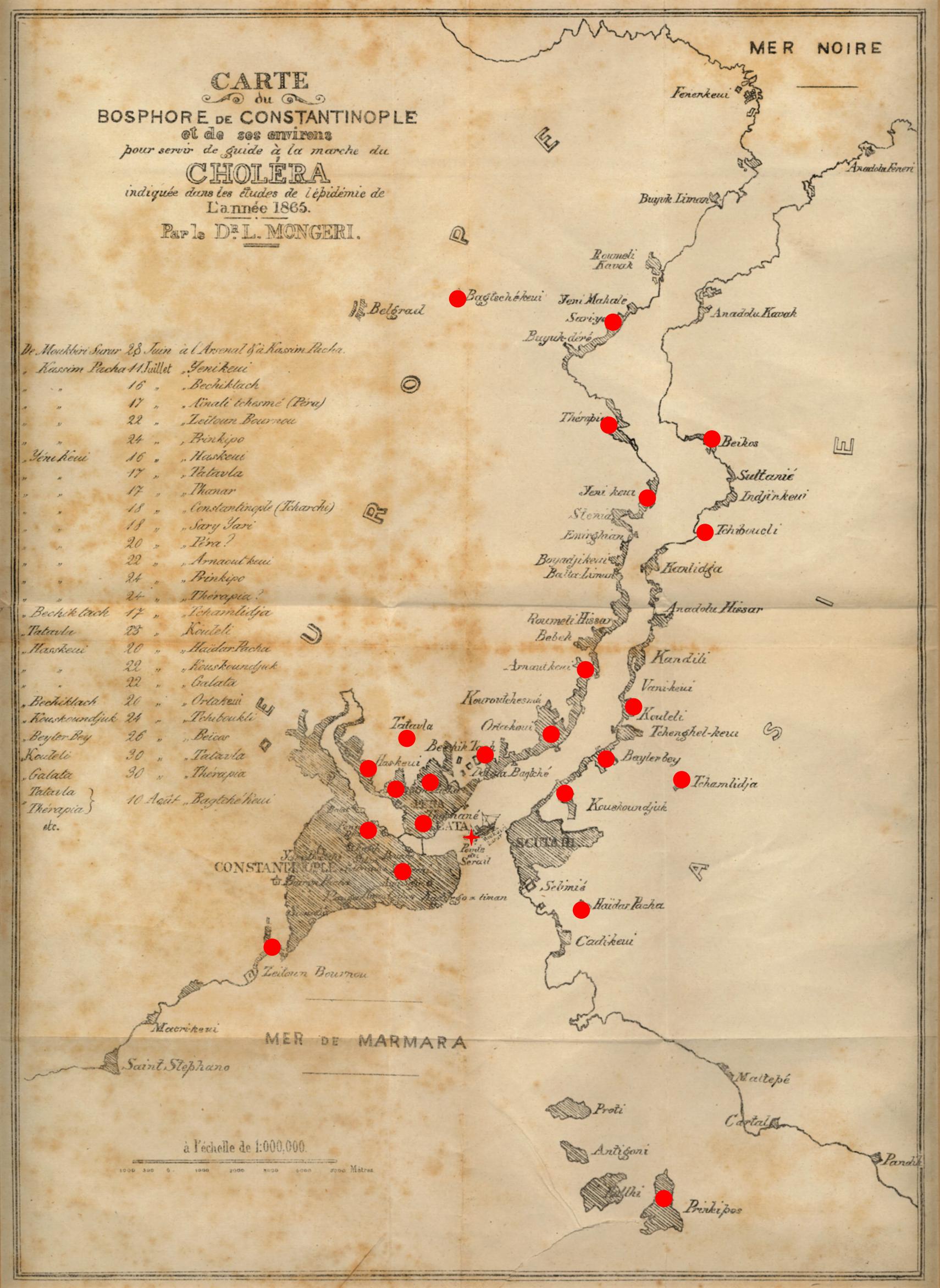
Map A map of Bosphorus and its surrounding areas drawn by Dr. Luigi Mongeri to explain the spread of the cholera epidemic in 1865. This map was attached to the last page of Mongeri’s book (Etudes sur l’Epidémie de Choléra qui a Régné à Constantinople en 1865, Constantinople: Imprimerie M. De Castro, 1866). The coloured version of the map above is from SALT Research Center- Sinan Kuneralp Collection.
Mongeri endeavoured for the construction of a modern asylum outside of the city walls of Istanbul on a large estate; however, when he understood that this was not going to happen, he moved the institution to Valide Atik Hospital in Uskudar’s Toptasi district, a relatively tranquil area in the city (14). So Toptasi Asylum is a product of a thought that flared up at the moment of danger. It is an institution that came into being as a result of persuading the state that the old institution had to be evacuated and moved to somewhere else urgently.
New Epidemics, Old Patterns
When Mongeri died in 1882, his assistant Dr. Avram de Castro took over his position (20). During his time as the Chief Physician, a cholera epidemic erupted in Toptasi Asylum in 1893. A total of 86 people died in a month (14). As the cholera epidemic took Istanbul hostage, some people pointed to the mental patients of the Toptasi Asylum as the reason for this epidemic. The justification they provided for this was the lack of sanitary habits of the mental patients, their lack of care for cleanliness, etc. So there was an attempt to somehow stigmatize them or at least look for a scapegoat.
Moreover, while the epidemic was raging and claiming lives, an asylum was set up in Yassiada by using barracks. A commission was set up, and investigations were made so as to move the entire institution to this place with all of its patients (14). Fortunately, this crazy project was abandoned at the last minute. The person who persuaded the other members of the commission to deter from the transfer decision was Celalettin Muhtar Özden, who had training and laboratory experience at Pasteur Institute. He was of the view that the safest way for the civilised states to eliminate cholera was to eradicate it at its place of origin (6, 14).
Mental asylums and prisons were easy targets as deadly outbreaks of cholera spread across the globe in five major pandemic waves during the 19th century. Cholera outbreaks in these institutions were spreading rapidly, resulting in high mortality among prisoners and patients already in poor states of health (21).
In the upcoming years, a few small-scale cholera epidemics broke out in Toptasi. The last Chief Physician of Toptasi Asylum, Mazhar Osman, began to move this institution to the derelict Reşadiye Barrack in Bakırkoy at the end of 1924, and Bakırkoy Psychiatric Hospital was found (14). Lastly, when the cholera epidemic broke out in Sagmalcılar in 1970, spread to Bakırkoy Hospital, the institution once more lost many people. Sagmalcılar cholera epidemic is one of the important events of Turkey’s recent health history, and it has especially left lasting traces in the minds of Istanbulites.
In 1978, the name Sagmalcılar was replaced with Bayrampasa in an attempt to erase the effect of cholera on people’s minds (22). The official records of the Parliament in 1971 mention the criticisms against the government and ministry on the handling of Sagmalcılar Cholera outbreak. Some of these criticisms included, “Not taking the required measures beforehand, not implementing quarantine, and taking delayed action for intervention” (23).
During Sagmalcılar cholera epidemic, we have heard from the witnesses of that period through oral history studies that more than 100 people died in Bakırkoy Psychiatric Hospital in a short time. The hospital staff told that they did not know how to behave during the cholera epidemic. They stated that they were not able to do anything other than putting tens of dead bodies that came from the wards each day to milk trucks so as to keep them away from people’s eyes and bury them in common graves (14). When considered together with what Mongeri wrote and experienced, it shows the importance of the memory regarding epidemics and that we need to think about them again. It also illustrates the graveness of the problem concerning the lack of institutionalisation when it comes to epidemic experiences and their management.
Conclusion
As I have pointed out earlier in the article, there are biological and epidemiological differences between COVID-19 pandemic and cholera epidemic. However, we can identify the similarities and common grounds, especially regarding social and political aspects, between these two outbreaks through Mongeri’s fundamental findings.
Firstly, epidemics and pandemics are not merely medical phenomena; the spread and control of the disease is mostly related to the political economy. Two keywords, time and money, are still dominant in describing the modern world that we live in. During the period that Mongeri lived in the 19th century, the limits of commercial greed were probably constrained with the intolerance of the merchants and capitalists for losing money and their desire to maintain their benefits uninterruptedly and increasingly. The capitalist greed of the 21st century, on the other hand, was set to work with a great appetite without losing any time as soon as it heard the term pandemic. The basic items, such as masks and sanitizers, which people would need most in such a pandemic, have been stored and sold for exorbitant prices. The national and international companies that are utterly intolerant of the slightest loss of profit have pressed for and are still pressing for the immediate, and if possible, wide opening of the doors of transportation, circulation, shopping, and consuming of the capitalist economy. But what about the consumerist individuals and societies, acting as natural extensions of the capitalist world? Have they behaved any differently? Hoarding has been frequently observed during the pandemic. The images of “panic buying” represented by the rush for acquiring large amounts of toilet paper are still vivid in our memories.
Secondly, different emotional stress, reactions and attitudes have emerged during epidemics and pandemics not only among people but also among physicians. As Mongeri wrote, “On the one hand, there is ignorance and lethargy resisting all measures that could effectively ward off disaster, and on the other hand, there are prejudices and habits that can preach futile practices, inspired by senseless fear.” These are two basic attitudes in the struggle with each other. These fundamental findings of Mongeri have been frequently voiced during the pandemic that we have been experiencing.
Thirdly, epidemics or pandemics are also a psychological phenomenon, maybe even more so. During the pandemic, is it possible not to talk about psychological contagion, more precisely the contagion psychology, along with the bodily or physical contagiousness? The physical disease has its pathogens, disseminates through vectors, follows the modes of transmission, ferments during the incubation, and erupts to overpower the host. Similarly, the public, psychological aspects of the outbreak have kernels of misinformation, feed on uncertainty, and grow in doubt as they incubate in the limbic system. And then, through vectors of media and communication, these aspects explode in the form of individual or mass panic, threatening to overpower the coping resources of an individual or an entire community (24).
In social psychology, one form of infectiousness is rule-violation contagions. Mongeri underlines that “sanitary rules are often violated in Lazarets”, and today we witness the violation of quarantine measures, such as lockdown, wearing masks, and social distancing rules.
According to clinical psychologist, Steven Taylor, “pandemics were not simply about some virus infecting people; pandemics were caused and contained by the way people behaved” (25). Pandemics are controlled only when people agree to do particular things, such as covering their coughs, washing their hands, and complying with social distancing rules. For various psychological reasons, if people refuse to do these things, then the pandemic will continue to spread (26).
Finally, epidemics and pandemics are not immune to the relationship between science and policy on the national and global levels. Of course, each pandemic is different, but as Alex de Waal underlines, “The logic of political action is much the same.” He also states, “Where political interests align with scientific advice, that advice becomes policy” (27).
In the time of Mongeri, his efforts to combat the cholera outbreak were not supported by the government and authorities. Anti-contagionism was strong not only among the medical circles but also among the rulers and politicians whose decisions mostly depended on the interests of the economy. The real issues were not only concerned with the theories of disease transmission, but were also economic, bureaucratic, political, and legislative. The application of those measures in some countries eventually led to a battle between liberals and conservatives around the issues of individual freedom and freedom of commerce. In some cases, preventive measures, such as quarantines and sanitary cordons, were increasingly portrayed as barbaric and medieval (28).
By the time cholera arrived in Europe, anti-quarantinists had condemned quarantine as “useless, a nuisance to trade, and obnoxious to growth” (29, 30). In relaxing lockdowns, European authorities also gave in to pressure from merchants, traders, and manufacturers. Today, we are not discussing the infectious nature of the disease, but the policies of the governments related to lockdowns, quarantine measures, and objections based on “anti-contagionism” to these practices. In conclusion, we are not only suffering from a real virus but also suffering more from politics all around the world. Therefore, it might be a historical moment when learning from the history of epidemics means learning from past and present politics.