Introduction
Anthrax is an acute zoonotic disease caused by the Gram-positive bacillus Bacillus anthracis, which primarily affects herbivores (1). It manifests as cutaneous, gastrointestinal, or respiratory anthrax, depending on the route by which the bacteria enter the body. Cutaneous anthrax often occurs during the handling of infected animals, while the gastrointestinal and pulmonary forms result from consuming contaminated meat or inhaling spores. Livestock breeders, butchers, and veterinarians are particularly at risk (2).
In Türkiye, particularly in eastern Anatolia, anthrax is endemic; however, its incidence is gradually decreasing, with annual cases falling below 300 since the 1990s (3-5). Approximately 95% of human cases are cutaneous and usually present on exposed skin areas, such as the face and neck, where significant edema can develop, potentially leading to respiratory distress (4, 6, 7). In this case report, malignant edema complication of cutaneous anthrax was presented to draw the attention of our clinicians because it is not a common clinical presentation; a patient presenting with angioedema symptoms was described.
Case

Figure 1. The patient presented with edema on the lips and the left half of the face, extending to the point of eyelid closure, and a hyperemic, insect bite-like papule approximately 1 cm in diameter on the left cheek at the edge of the lip (Day 1).
A 44-year-old woman from Bahçesaray, Van, presented to the emergency department with facial wounds and edema. She reported working with sheep and cows and having no pain from insect bites. However, upon waking, she noticed swelling and a wound on her face. Examination revealed significant edema on her lips and the left side of her face, along with a painless, hyperemic papule on her cheek (Figure 1). Additionally, there was a black, crusted wound with a diameter of approximately 0.5 cm on the distal third finger of the right hand that appeared three days earlier.
Her medical history included asthma, and her vital signs were stable at admission (temperature: 36.5°C, oxygen saturation: 98%, pulse: 67 bpm, and blood pressure: 100/60 mmHg). Initial laboratory evaluation revealed a white blood cell (WBC) count of 6,000/mm³, C-reactive protein (CRP) level of 5.5 mg/L (reference range: 0–5), lymphocyte count of 900/µL, aspartate aminotransferase (AST) of 75 U/L, and alanine aminotransferase (ALT) of 72 U/L; all other parameters were within normal limits. The condition was initially suspected to be an allergic reaction, and she was treated with prednisolone and pheniramine. However, due to worsening symptoms, including difficulty swallowing, adrenaline was administered.
During the follow-up in the ward, the patient was administered adrenaline (0.5 mg) intramuscularly twice due to difficulty swallowing and laryngeal edema; however, the patient was followed up again after experiencing partial relief. The next day, the edema on the face worsened, and her difficulty swallowing continued. She was referred to our allergy and immunology service in Van with a preliminary diagnosis of bradykinergic angioedema.
Given that the edema did not respond to adrenaline, antihistamine, and systemic corticosteroid treatment and that her oxygen saturation decreased from 98% to 93%, she was treated for an acute laryngeal edema attack due to bradykinergic angioedema with intravenous C1 esterase inhibitor (C1-INH, Cinryze® 1000 IU, Takeda Pharmaceuticals International AG, Switzerland) (8). However, there was no regression in the patient’s angioedema.

Figure 2. It was observed that the wound on the face had turned into a vesicle and looked like a dark-colored superficial ulcer and facial edema (Day 2).

Figure 3. The patient also had a black crusted wound with a diameter of approximately 0.5 cm on the distal third finger of the right hand (Day 2).
Upon re-evaluation by the allergy and immunology service, it was observed that the wound on the face had turned into a vesicle with the appearance of a dark-colored superficial ulcer (Figure 2). Additionally, the patient had a black crusted wound with a diameter of approximately 0.5 cm on the distal third finger of the right hand (Figure 3).
Superficial ultrasonography (USG) of the left facial region showed markedly edematous subcutaneous fatty tissue and lymphadenopathies extending up to 12 mm in the submental area. The neck ultrasound scan revealed 3-4 lymphadenopathies, with an increased bilateral submental region round index and inflammation of the surrounding fat planes, measuring 12 mm in diameter.
Following consultation with infectious disease specialists, she was diagnosed with cutaneous anthrax based on the appearance of her wounds. A wound aspirate sample was taken and inoculated on sheep blood agar and eosin methylene blue (EMB) agar. Gram staining of the sample obtained from the lesion demonstrated a polymorphonuclear leukocyte, but no microorganism was observed. On the same day, three blood culture samples were taken and incubated using an automated blood culture system (BacT/ALERT, bioMérieux, Durham, NC, USA). The real-time PCR test for B. anthracis resulted in a positive outcome. The results of the wound and blood cultures were negative.

Figure 4. One day after antibiotic treatment, the edema on her face started to recede (Day 3).

Figure 5. On the third day of antibiotic treatment, the edema subsided significantly (Day 5).

Figure 6. On the fourth day of antibiotic treatment, the edema subsided significantly (Day 7).

Figure 7. Two weeks after the end of treatment.
The patient was diagnosed with malignant edema, the most serious form of cutaneous anthrax. She was monitored as extubated in the intensive care unit. On the second day of hospitalization, intravenous meropenem (1 g three times daily) and ciprofloxacin (400 mg twice daily) treatment was initiated (9). One day after initiating antibiotic treatment, the edema on her face started to recede (Figure 4). On the third day (Figure 5) and fourth day (Figure 6) of treatment, the edema subsided significantly. On the seventh day, the patient’s edema completely regressed. A follow-up photograph taken two weeks after treatment completion is shown in Figure 7.
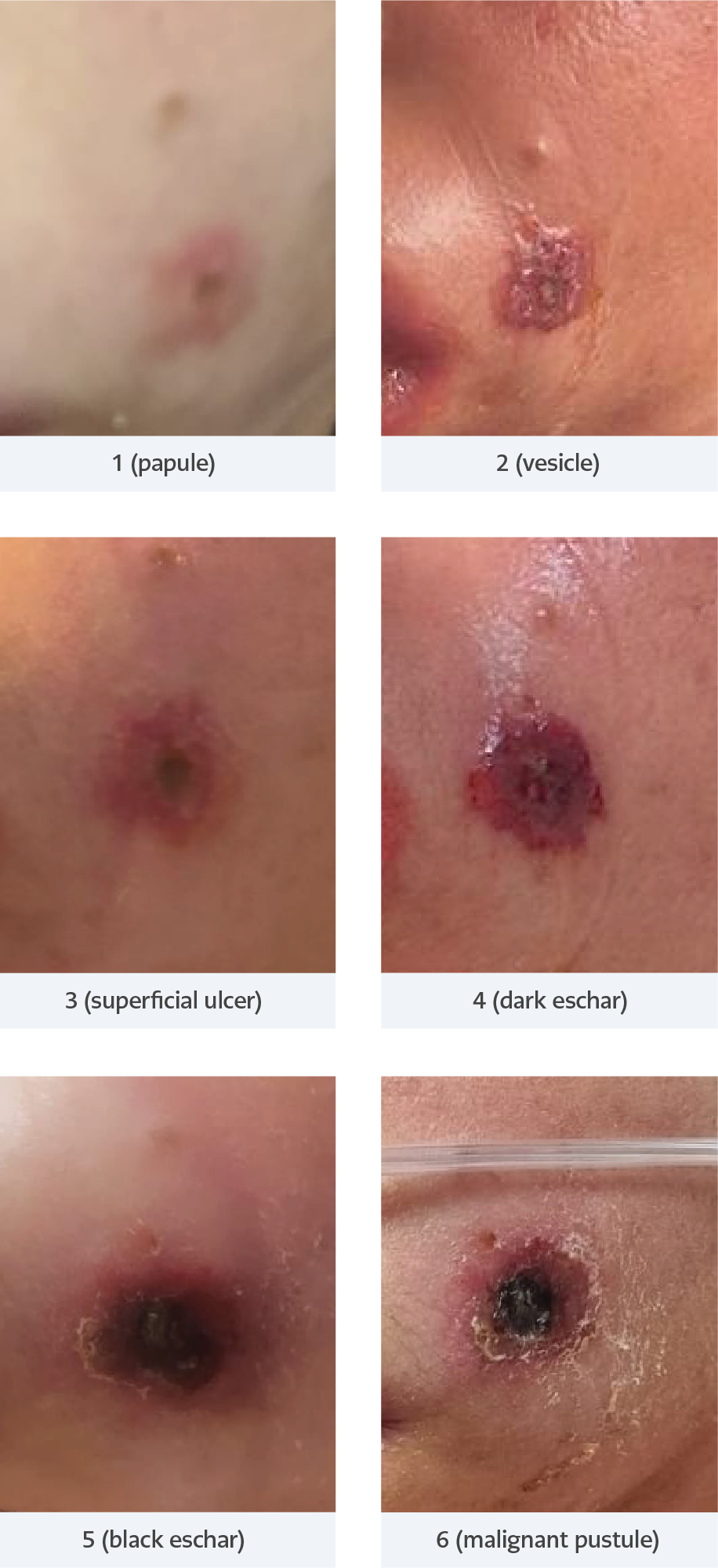
Figure 8. The course of the patient’s lesion over time.
The patient was reported to the local community health center as a case of anthrax. No additional cases of anthrax were identified among the patient’s family members or animals. The course of the patient’s lesion over time is illustrated in Figure 8.
Informed consent was obtained from the patient, who accepted the treatment and agreed to the publication of this case report, along with the accompanying photographs.
Discussion
This case emphasizes that anthrax is still endemic in regions where animal husbandry is common and should be considered in the differential diagnosis of patients presenting with facial angioedema. Cutaneous anthrax usually appears on naked parts of the body, such as the hands, arms, face, and neck. Our patient likely transferred the infection from the lesion on her hand to her face by scratching.
At the presentation, our patient had a typical painless anthrax vesicle. In a few days, the fluid inside the vesicle became cloudy and turned into a blue-black appearance. The vesicle burst, forming a black ulcer with a sunken center. Anthrax was considered for the patient involved in animal husbandry due to the highly characteristic necrotic ulcer with a black central eschar. Additionally, the patient developed painful regional adenomegaly in the neck. Cutaneous anthrax lesions are more commonly found on exposed areas, such as the head, neck, and extremities. Due to the accompanying itching, the painless lesion is often misidentified as an insect or spider bite (10). Therefore, such lesions should be monitored closely.
The bacterial culture method is the gold standard for diagnosing anthrax; however, positive culture results observed among patients do not exceed 65%. In addition, within a few hours after the first dose of penicillin, the culture of lesion samples may become negative (11). Our patient had not received antibiotics. Therefore, in such cases, clinical diagnosis based on the patient’s history and physical examination findings are important. Anthrax should be suspected in the presence of a painless necrotizing ulcer or a black eschar and edema with positive epidemiological data.
Our patient had toxemia, hypotension, and extensive malignant edema on the face and was monitored in the intensive care unit. Because of clinical findings of severe anthrax, broad-spectrum antibiotics, such as meropenem and ciprofloxacin, were administered. There was no growth in the culture, but broad-spectrum antibiotic treatment, such as meropenem, was continued because of the patient’s critical condition. In another case report, meropenem, ciprofloxacin, and linezolid were used to manage severe cutaneous anthrax (12).
Conclusion
Although the incidence of anthrax is declining, it remains a public health concern in endemic areas. Recognition of the signs and symptoms by physicians is important for early diagnosis and effective treatment of severe cutaneous anthrax. In patients with a history of close contact with livestock, anthrax should be considered in the differential diagnosis. Reporting cases is crucial for effective public health measures.