Introduction
Listeria monocytogenes is a rare, self-limiting cause of gastroenteritis in healthy adults. It is generally transmitted through foods such as meat, raw vegetables, milk, and dairy products (1). It can cause life-threatening invasive infections in pregnant women, newborns, the elderly, transplant recipients, and patients with an impaired cellular immune response (2-4). In this report, a geriatric case who presented with acute gastroenteritis and was diagnosed as Listeria bacteremia is presented.
Case Presentation
An 81-year-old female patient was hospitalized with complaints of nausea, vomiting, watery bloodless diarrhea accompanied by tenesmus approximately 20 times a day, dysuria, and pollakiuria for two days. Her anamnesis revealed that she had hypertension, hyperlipidemia and coronary artery disease, she lived with her sister and that her meals were regularly served from a restaurant.
Physical examination
She was conscious, her fever was 38 °C, her blood pressure was 90/70 mmHg, and her skin and mucous membranes were dehydrated. Hepatomegaly and suprapubic tenderness were detected.
Laboratory tests
Leukocytes 12,000 /mm3, aspartate aminotransferase (AST) 50 IU/ml, alanine aminotransferase (ALT) 55 IU/ml, urea 20 mg/dl, creatinine 0.8 mg/dl, C-reactive protein (CRP) 187 mg/L were detected. Plenty of leukocytes were seen in stool microscopy, and any pathogenic bacteria did not grow in the culture. In the complete urinalysis, leukocyte and nitrite positivity were detected. Escherichia coli 103 colony-forming unit (CFU)/ml sensitive to ceftriaxone grew in urine culture. Stool culture was cultured on blood agar, eosin-methylene blue agar and salmonella-shigella agar as a part of the clinical routine. Pathogenic bacteria did not grow in stool culture. Listeria monocytogenes was grown on the third day in the blood culture of the patient in two vials. Blood samples sent to the laboratory were examined with the BACTEC 9120 (Becton Dickinson, USA) automated blood culture system. Blood cultures that gave positive signals in the device were inoculated on 5% sheep blood agar, eosin-methylene blue agar and Sabouraud’s dextrose agar media. The catalase-positive, oxidase-negative colonies grown on blood media with gram-positive bacillus appearance were loaded into the VITEK® 2 (bioMérieux, Marcy l’Etoile, France) identification device. The strain identified as Listeria monocytogenes by the device was then confirmed by the matrix-assisted laser desorption-ionization time-of-flight (MALDI-TOF) mass spectrometry (Bruker Daltonics, Bremen, Germany).
Ultrasonography
Bilateral grade 1 hydronephrosis and pelvicalyceal ectasia were detected in the kidneys.
Clinical follow-up
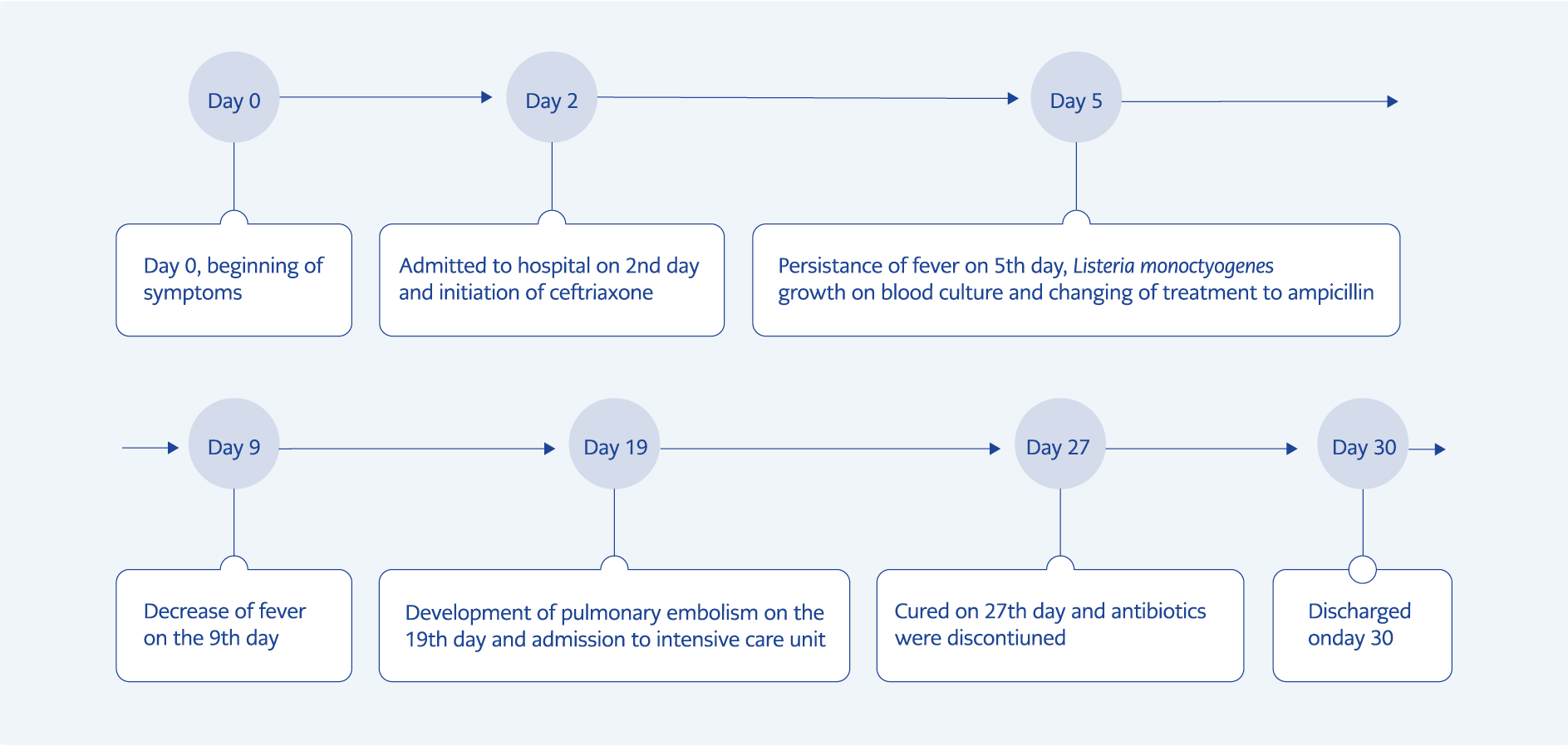
Figure 1. The timeline of the case, summary of the disease, symptoms, treatments, and complications.
Because during admission, the patient had a fever, leukocytes and nitrite positivity was detected in the complete urinalysis, urinary system infection was considered and intravenous (IV) ceftriaxone treatment was started. Listeria monocytogenes was grown on the third day in the patient’s blood culture, whose fever and diarrhea persisted despite appropriate treatment. The treatment was changed to ampicillin-sulbactam 4×2 gr IV. On the fourth day of ampicillin sulbactam treatment, the patient’s fever subsided. On the 14th day of the treatment, a pulmonary embolism developed despite the prophylactic low molecular weight heparin treatment, so she was transferred to the intensive care unit. The patient was followed up in the intensive care unit for six days, and the treatment was completed in three weeks (Figure 1). The patient, whose general condition improved, was placed in a nursing home with the support of the social service.
Discussion
In geriatric patients, infections may present with different clinical manifestations. Urinary tract infections and urosepsis are the most common infections in this age group. Therefore, if there are urinary symptoms, empirical antibiotic therapy is initiated for the urinary tract. Unnecessary antibiotic treatment in cases with asymptomatic bacteriuria is commonly seen in practice. This may cause the real infectious agent to be missed. Therefore, taking blood cultures from the cases is very important to prevent wrong approaches. A similar condition was experienced in the presented case, and ceftriaxone treatment was started because of urinary symptoms. The presence of ceftriaxone-sensitive Escherichia coli growth in the urine culture also supported the diagnosis. Listeria monocytogenes growth in the blood culture made it possible to recognize the presence of a different infection in the patient.
Listeria monocytogenes is an infectious agent transmitted by consuming contaminated food and can cause severe clinical presentations in immunosuppressive individuals, the elderly, and pregnant women (2). The gastrointestinal tract is the most important gateway. Foods made from unpasteurized milk, ready-to-eat, and frozen foods, especially ham, sausage, hot dog, chicken salad, and roast beef have been reported as risky foods (5). Food not prepared in proper conditions, poor storage conditions after preparation, and personnel working in food preparation play an important role in contamination. The fact that the presented case constantly consumed food from a restaurant is a significant risk factor for transmission.
The microorganism often causes central nervous system and bloodstream infections. Listeria monocytogenes does not produce any enterotoxin, and its molecular pathogenesis is not clearly known. It is phagocytized by attaching to the host cell with e-cadherin. It has been shown to cause invasive diarrhea, fever, and bacteremia (6, 7). As in our case, acute enteritis may occur either as the sole symptom of Listeria infection or as a finding preceding typical manifestations such as sepsis, meningitis, and encephalitis. A rare complication of Listeria gastroenteritis may lead to severe sepsis and death (2). This condition reveals the importance of taking blood culture in cases presenting with diarrhea, especially in the geriatric age group.
In patients who have diarrhea accompanied by fever, bloody or mucoid stools, severe abdominal cramps or tenderness, or sepsis symptoms, a stool test should be performed for Salmonella spp., Shigella spp., Campylobacter spp., Yersinia spp., Clostridium difficile and Shiga toxin-producing E. Coli (STEC). If enteric fever or bacteremia is suspected, culture-independent diagnostic testing, including panel-based multiplex molecular diagnosis from stool and blood samples, should be performed when indicated. In addition, bone marrow cultures (especially valuable if antimicrobial agents have been administered), stool, duodenal fluid, and urine may be useful in detecting enteric fever (8). However, in our case, only stool sample was cultured on blood agar, eosin-methylene blue agar, and salmonella-shigella agar as a part of the routine, and blood culture was taken for bacteriology because of the fever.
Empirical antimicrobial therapy is recommended in immunocompromised patients with febrile or bloody inflammatory diarrhea (8). In addition, it is recommended that in risk groups for severe listeriosis, such as the elderly, pregnant women, newborns and immunocompromised hosts, gastroenteritis should be treated with ampicillin or trimethoprim-sulfamethoxazole in case of diarrhea.
In a study examining two hundred and twenty-nine Listeria cases, it was reported that cephalosporins were used in 90% of undertreated cases. In the study, it was observed that 195 patients who survived were given adequate and appropriate antibiotic therapy in the early period (9). Similarly, in our case, empirical cephalosporin was started, and no improvement was observed. Mortality of Listeria infection has been reported as 26.6% and 38% in different studies (9, 10). Early diagnosis and appropriate treatment are lifesaving. Penicillin or ampicillin appears to be the first-choice drug in Listeria treatment (11-13). Depending on the clinical presentation, gentamicin can be added to the treatment. Severe listeriosis infections should be treated with a combination of ampicillin + gentamicin.
Ceftriaxone is not a good option in the treatment of cases (11). In our patient, fever response could be achieved on the seventh day of the disease by changing the treatment to ampicillin sulbactam.
Cases with Listeria bacteremia should be followed closely for the clinical manifestations, including pneumonia, peritonitis, and septic pulmonary embolism, which may be caused by Listeria (14, 15), and if possible, severe cases should be followed up under intensive-care conditions.
Conclusion
Special attention should be paid to patients’ nutrition in the geriatric age group, unpasteurized dairy products should be avoided, and ready-to-eat food consumption should be limited if possible. In addition, it should be kept in mind that in this age group, infections may present with different clinical manifestations and Listeria may be among the infectious agents, and blood cultures should be taken from all cases with fever.