Introduction
Crusted scabies, also called Norwegian scabies, was first described in Norway in the middle of the 19th century. It is a highly contagious and rare form of scabies. Patients who are elderly, immunocompromised, malnourished, or have neurologic conditions that prevent them from itching are at greater risk. It is characterized by vesicles and thick crusts over the skin that contain millions of Sarcoptes scabiei mites. Although the predominant route of transmission is skin-to-skin contact, crusted scabies can be transmitted indirectly via patients’ bedding, clothes, or surroundings, and can cause outbreaks in institutional settings or nursing homes. Here, we report a case of Norwegian scabies in an elderly patient who resided in a nursing home (1-3).
Case presentation
An 88-year-old female resident of a care home was admitted to our intensive care unit with fever and respiratory distress. The patient had been bedridden for two years and had chronic obstructive pulmonary disease and dementia diagnoses. On admission, she was confused, in a generally poor condition and asthenic. Her body temperature was 37.8o C, pulse rate 94 beats/min, blood pressure 90/60 mmHg, respiratory rate 25/min, and SpO2 90% at room temperature. Upon physical examination, she was noted to have hyperkeratotic plaques with yellow crusts on the scalp, face, hands, and feet (Figure 1-4). A respiratory examination revealed crepitation in both lower lungs. Other system examinations were unremarkable.
Laboratory analysis revealed leukocytosis (19600/mm3), polymorphonuclear leukocyte (94.7%), anemia (Hb:9 mg/dl, Hct:32.4), thrombocytopenia (60000/mm3), hypoalbuminemia (1.8g/dL), hyperchloremia (120.6 mmol/L), hypernatremia (151 mmol/L), azotemia (creatinine: 2.04 mg/dL), elevation of C-reactive protein (246.7mg/L) and procalcitonin (5.85 ng/mL). Viral serologic markers for hepatitis B, hepatitis C, and HIV were negative. A chest X-ray showed consolidation in the middle lobe of the left lung. Blood and urine cultures were collected. Antimicrobial therapy (ceftriaxone and clarithromycin) were empirically started.

Figure 1-4. Erythematous papules and vesicles, hyperkeratotic plaques and papules primarily on the scalp, face, hands and feet.
A dermatology consultation was performed for the cutaneous findings and keratotic plaques on the scalp, face, hands, and feet. The widespread excoriated scaly eruption, papules, and vesicles on the body were detected. A potassium hydroxide microscopic wet-mount examination of the skin scales showed scabies mites and eggs (Figure 5). Norwegian scabies was diagnosed with clinical and microscopic findings.
Urgent isolation measures (contact precautions) were taken by the hospital infection control team, according to the Centers for Disease Control and Prevention protocol, to avoid nosocomial transmission (4). Intensive care unit personnel were rapidly trained about scabies and infection control measures. Personal protective equipment (gloves, long-sleeved gowns, shoe covers, surgical masks) and hand hygiene compliance of the staff providing care to the patient were ensured. The bedding of the patient was transported in a plastic bag and washed in a separate washing machine at over 60o C. Also, the laundry personnel used personnel protective garments when handling the laundry. The patient’s room was cleaned regularly for skin crusts that can contain a large number of mites. Intensive care unit caregivers were advised to bathe every day with sulphur soap.
The dermatologist recommended a pharmacological treatment of the patient with oral (ivermectin tab 200 µg/kg PO one dose and repeated after one week) and topical medication (salicylic Vaseline 15% between fingers 2 × 1; scalp rubbing with oil and limestone ointment at night, and washing with sulphur soap in the morning; precipitated sulphur 30 gr + cade oil 20 gr + lanoline 60 gr + Vaseline 90 gr applied on her entire body every night, and washing with sulphur soap every morning for four consecutive days) simultaneously. We observed regression after treatment (Figure 6). However, the patient died of pneumonia on her fifth day of hospitalization due to her advanced age and comorbidities. Klebsiella pneumoniae was isolated in the endotracheal aspirate. The Communicable Disease Control Unit was notified that a patient from the nursing home had been diagnosed with Norwegian scabies.

Figure 5. Regression of the lesions on the face after treatment.
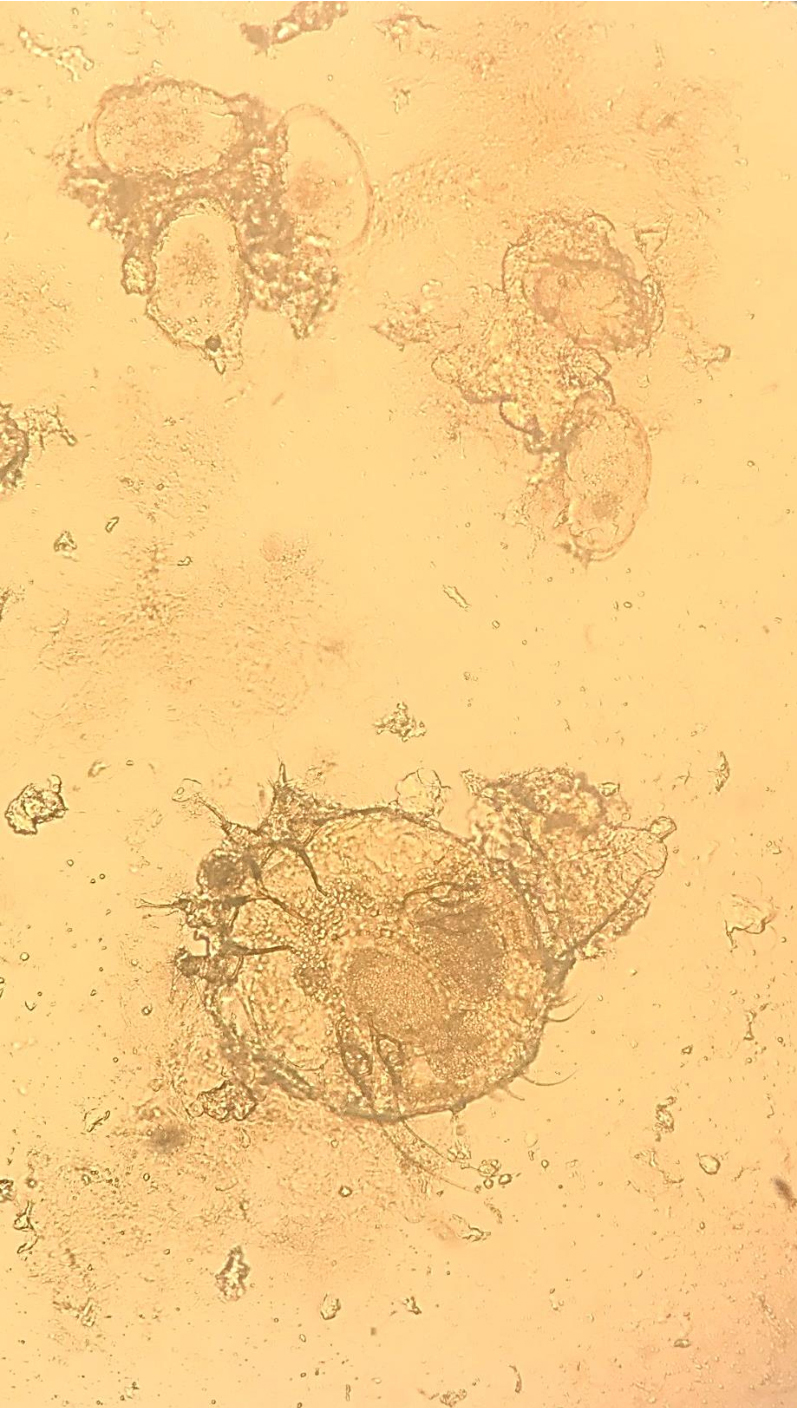
Figure 6. Scabies mite and eggs under light microscopy (mounted in KOHX400).
Discussion
Half of the patients with scabies who live in nursing homes do not exhibit the typical signs and symptoms, as the disease progresses asymptomatically. Scabies outbreaks are common in these institutions because of delayed diagnosis and the demanding effort required to control infection. Norwegian scabies, specifically, has a huge mite burden, is highly contagious, and can cause epidemics in these long-term care facilities (5-7). Factors that predispose an individual to crusted scabies include immunosuppression, neurological diseases, advanced age, malnutrition, and institutionalization (7-9). In our case, advanced age, malnutrition, and dementia were the main risk factors that caused a reduced ability to control the proliferation of the mites.
The diagnosis of scabies is made clinically, but definitive diagnosis is based on a low power microscopic examination of a burrow skin scraping. In Norwegian scabies, as crusts contain large numbers of mites and eggs, diagnosis can be made easily with excellent specificity and sensitivity. However, in classic scabies, sensitivity is low due to low numbers of mites. Also, an increased number of scrapings, sampling of unscratched lesions and experience of the individual performing the examination are factors that increase sensitivity. Histopathological findings may also confirm the diagnosis (3,10). Among the diseases that should be taken into consideration in the differential diagnosis are psoriasis and atopic dermatitis, especially in elderly patients (2). Although no standardized protocols are available, treatment includes keratolytic agents besides topical and oral scabicides because of the high mite burden and hyperkeratotic lesions of the crusted scabies. Ivermectin is the systemic drug of choice (7).
Conclusion
Considering that the number of people who require care in a nursing home is increasing with the aging world population, infectious diseases, such as scabies, will continue to be among a considerable public health issue in this age group. Norwegian scabies disease is commonly documented in nursing homes, as in our case. Healthcare workers should be aware of this form of scabies, which is highly contagious and seen more common in elderly and cognitively impaired patients. Therefore, early diagnosis, which can be made easily by microscopic examination of skin lesions and isolation precautions, are important measures to prevent outbreaks in both settings.