Introduction
Polymerase chain reaction (PCR) test is used in high-capacity laboratories in the diagnosis of COVID-19. On the other hand, rapid SARS-CoV-2 antigen tests require less technical expertise and laboratory capacity. Antigen tests, which are faster and cost-effective, are increasingly used in COVID-19 screening and diagnosis (1). This study aimed to compare the i-test COVID-19 rapid antigen test (Sentromer DNA Technologies, Inc., İstanbul, Türkiye) and SARS-CoV-2 reverse transcriptase PCR test in symptomatic COVID-19 suspected patients.
Materials and Methods
We included 200 consecutive patients admitted to Bursa Uludağ University Hospital Pandemic Outpatient Clinic with respiratory infection symptoms. A patient with at least two symptoms of fever, cough, sore throat, headache, myalgia, loss of smell or taste, and runny nose that lasted less than a week were included in the study. Together with the patient’s contact history, two combined oro/nasopharyngeal swabs (FLOQSwabs®; Copan, Brescia, Italy) samples were collected by healthcare workers between April and June 2022. One of the swab samples was transferred to the laboratory in a viral nucleic acid transport (VNAT) medium, which was used for RT-PCR, and the other swab was sent to the laboratory in a sterile tube, which was used for antigen testing.
We used i-test COVID-19 rapid antigen test v1 (Sentromer DNA Technologies, Inc., İstanbul, TÜrkiye), an immunochromatographic test resulting in 10 minutes and SARS-CoV-2 RT-PCR test kit (Laborant SARS-CoV-2 RT qPCR; Ant Medical, İstanbul, TÜrkiye) for detecting SARS-CoV-2.
All experiments on human participants were performed in accordance with the Declaration of Helsinki, and all participants provided written informed consent. The protocol was approved by the Uludağ University Faculty of Medicine Clinical Research Ethics Committee on March 30, 2022 with approval number 2022-7/22.
We statistically analyzed sensitivity, specificity, and overall agreement. We used Fisher’s exact test with or without Yates correction and Pearson’s Chi-square test. The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 23.0 (IBM Corp., Armonk, NY, USA).
Results
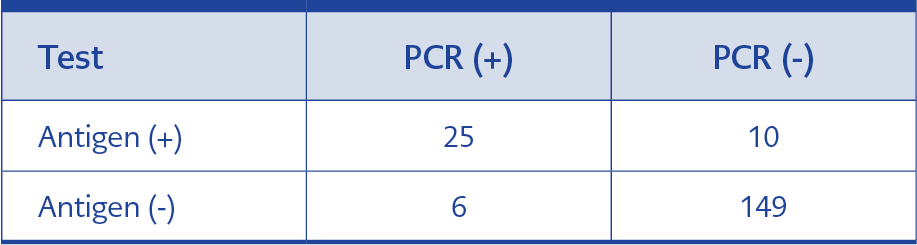
Table 1. Antigen and PCR test results for negative samples and PCR positive samples with a Ct value <30.
The mean age of the 200 patients included in the study was 35.82. Ninety-four (47%) of the patients were male, and 106 (53%) were female. The PCR tests of 41 of the patients were positive, and 159 were negative. The cycle threshold (Ct) values of the patients were found to be between 21.6 and 34.4. The Ct value of 10 patients with positive PCR tests was >30. It was found that the sensitivity and specificity of the antigen test were 80.6 % and 93.7 %, respectively, for samples with a Ct value of <30; overall agreement between antigen and PCR test was 91.6 % for these samples (Table 1) (Ten tests that have Ct value>30 were not included in Table 1). Positive predictive values (PPV) and negative predictive values (NPV) were 73.5 % and 95.9 %, respectively. When the analysis was performed on all patients with positive results with PCR, sensitivity, specificity, and overall agreement of tests were calculated as 75.6%, 93.7%, and 90%, respectively. The patients were evaluated for contact history and symptoms of fever, cough, sore throat, headache, myalgia, loss of taste and smell, and runny nose. The sore throat was the most common symptom in all of the patients. Myalgia was the second most frequent symptom in the test-positive group. The runny nose was the second most frequent symptom in the test-negative group. There was no significant difference between the PCR positive and negative groups in symptoms of fever, cough, sore throat, and headache. Loss of taste and smell, myalgia, and contact history were statistically more frequent in the group with positive PCR and antigen tests. There were 10 patients whose PCR tests were positive but antigen tests negative. Seven of these patients had myalgia, six had a sore throat and headache, and four had a runny nose. The runny nose was statistically more frequent in the negative group.
Discussion
Rapid antigen tests are increasingly used in COVID-19 screening and diagnosis. There is a large gap in performance data for symptomatic adults and asymptomatic adults and children due to the need for knowledge of how to perform rapid antigen testing optimally and the inability to perform all these tests equally in comparative studies (2). The World Health Organization (WHO) recommends using rapid antigen tests in adults with onset of symptoms less than seven days and, if the result is negative, confirm the results by RT-PCR or repeat the test. In addition, during the pandemic, the trend in disease incidence, isolation, and screening for early detection of the disease was recommended to be monitored through rapid antigen tests (3).
The results of PCR and i-test COVID-19 rapid antigen test v1 were compared according to symptoms of patients and the symptoms related to COVID-19, like myalgia and headache, which were more common in PCR (+) and antigen (-) patients. As myalgia was statistically more common in the PCR and antigen (+) group, we argue that myalgia-positive patients in the PCR (+) and antigen (-) group reveal the fact that the sensitivity of the PCR test was better than the i-test COVID-19 rapid antigen test. Krüttgen et al. used 75 swabs from positive patients by SARS-CoV-2 PCR and 75 swabs from negative patients by SARS-CoV-2 PCR and investigated the sensitivity and specificity of the SARS-CoV-2 Rapid Antigen Test (Roche, Basel, Switzerland); they found the assay’s sensitivity with samples with a cycle threshold of < 25 as 100%, 25 – 30 as 95 % and 30-35 was 44.8 % (4). Krüger et al. compared the rapid antigen test (Sure Status®; PMC Private Limited, Sarigam, India) and RT-PCR test results in Germany and India; the sensitivity was 82.4 %, and the specificity was 98.5 % (5). Tamura et al. investigated symptomatic COVID-19 patients to study the diagnostic accuracy of a novel SARS CoV-2 rapid antigen test and showed the sensitivity of the antigen test 100% for the first six days of the disease using specimens with moderate or high viral load (Ct value <30); however, from day 7, the sensitivity was 70.4-90.6 % and 83.9-84.6 % for the anterior nasal and nasopharyngeal sites, respectively (6). Besides nasopharyngeal samples, gargle and mouthwash samples can also be used for diagnosis (7).
During the pandemic and our study, respiratory viruses other than COVID-19 also caused respiratory tract infections (8). Although the symptoms of respiratory tract infections are similar to each other, tests to determine the causative agent should be performed for differential diagnosis, and physicians should follow viral surveillance (9). Antigen tests may become favorable because they do not need expensive equipment or trained personnel and usually result in 15 minutes.
In conclusion, although the PCR test has a better performance on sensitivity and specificity, the i-test Covid-19 rapid antigen test can be used for screening in schools, factories, and nursing homes and for diagnosis in health centers where PCR tests are unavailable.