Introduction
Nocardia is a genus of aerobic, Gram-positive bacteria found in soil, decomposing organic matter, and water. It primarily causes infections in individuals with compromised immune systems. Pulmonary infections represent the most frequent manifestation of Nocardia-associated diseases, while extrapulmonary spread often involves the brain, skin, and soft tissues (1). Central nervous system (CNS) infections typically arise from hematogenous spread, most commonly presenting as brain abscesses. In contrast, Nocardia-induced meningitis and ventriculitis are rare (2).
Ventriculitis is an uncommon infectious condition affecting the ventricular ependymal lining (3). Diagnosis is typically made through magnetic resonance imaging (MRI), revealing intraventricular debris, pus, or periventricular abnormalities (4). Reported cases of primary Nocardia-induced ventriculitis are few, and Nocardia otitidiscaviarum is an especially rare causative agent.
Case
A 64-year-old woman presented with a three-week history of worsening headache, confusion, and weakness. She had a history of idiopathic thrombocytopenic purpura and had been started on methylprednisolone 80 mg/day five months earlier, which was tapered and discontinued two weeks prior to admission.
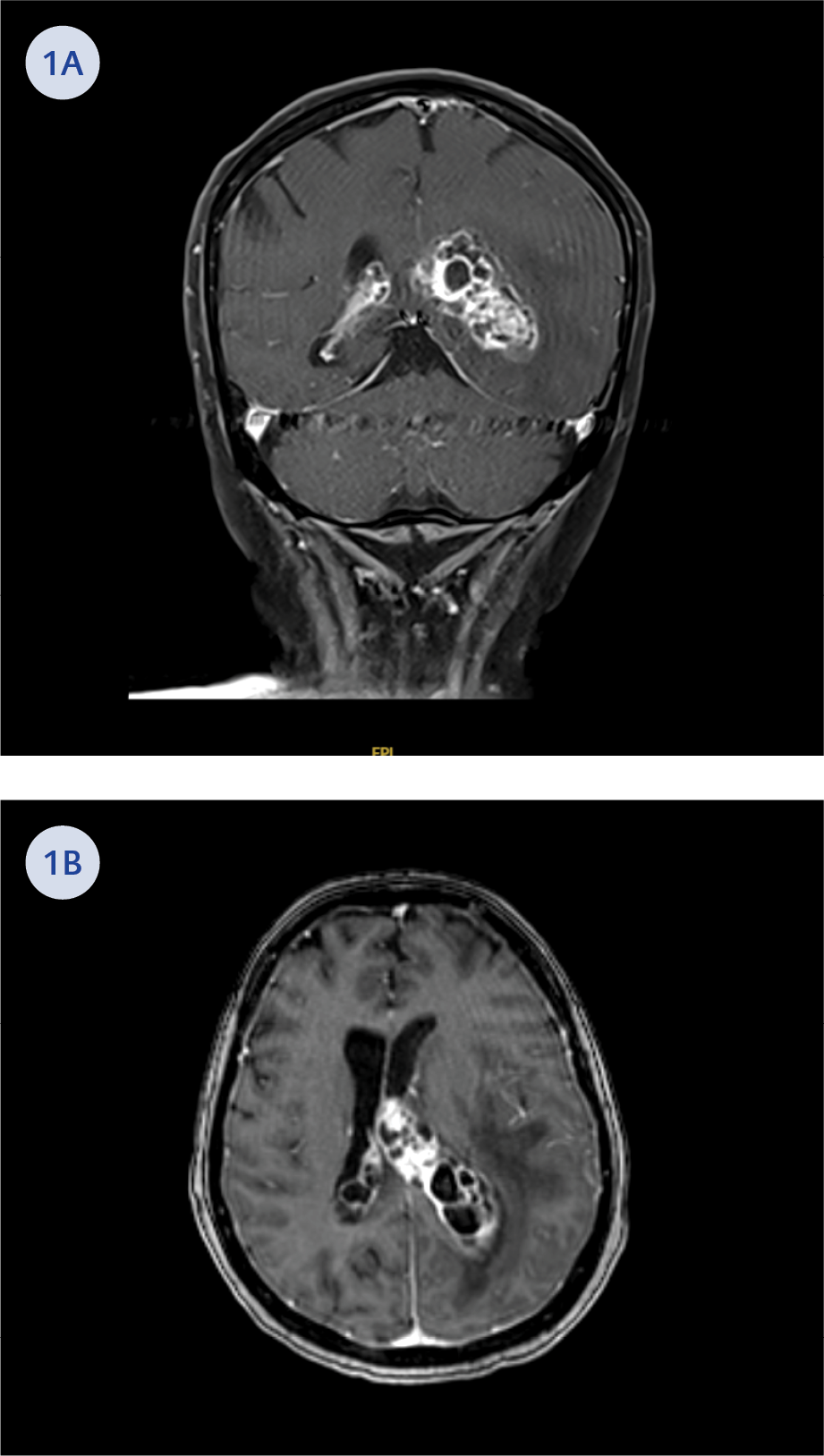
Figure 1. T1-weighted magnetic resonance imaging (MRI) findings. Coronal (A) and axial (B) T1-weighted MRI images demonstrate dilatation of both lateral ventricles and the presence of multiple cystic lesions with peripheral contrast enhancement.
On presentation, the patient was lethargic, disoriented, and had a Glasgow Coma Scale (GCS) score of 13. She was afebrile, and there were no signs of meningeal irritation. Initial laboratory tests revealed leukocytosis, neutrophilia, and elevated C-reactive protein (CRP) levels. Cerebral MRI showed asymmetrically enlarged lateral ventricles and increased cerebrospinal fluid (CSF) signal, suggestive of infection. The choroid plexus was enlarged, and cystic lesions with peripheral contrast enhancement were detected along the ependymal lining, starting from the left posterior lateral horn and extending to the left temporal horn. There was a minimal (3 mm) midline shift to the right. Additionally, a 1 mm diameter right cerebellar contrast-enhancing lesion was noted. These findings were consistent with choroid plexitis, ventriculitis, and ependymitis of infectious nature (Figure 1).
Cerebrospinal fluid analysis revealed a leukocyte count of 0.698×10³/μL, with no erythrocytes. The protein concentration in CSF was measured at 282.1 mg/dL. Serum glucose level was 232 mg/dL, and CSF glucose level was 54 mg/dL. Aerobic and fungal cultures, as well as multiplex PCR tests for viral and bacterial pathogens, yielded negative results. Nocardia was not isolated from the CSF cultures.
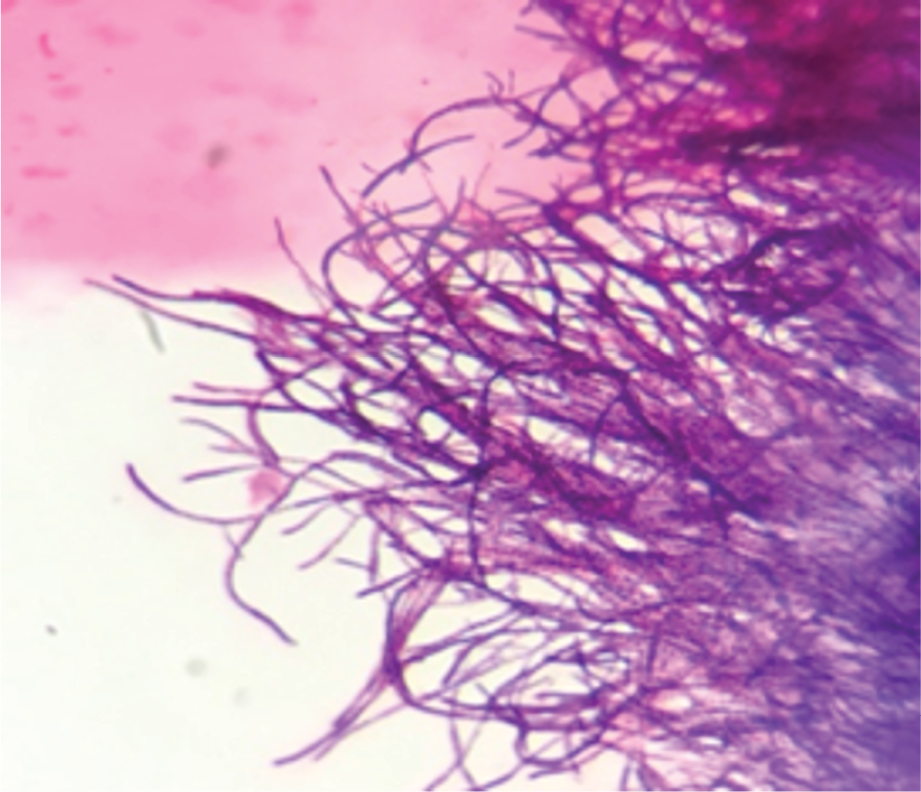
Figure 2. Gram stain of the intraoperative pus culture revealed filamentous, branching Gram-positive bacilli consistent with Nocardia.
Empirical therapy with meropenem, vancomycin, and dexamethasone was initiated. Six days later, the patient’s GCS score dropped to 5, prompting emergent surgical intervention. Purple multilobular and cystic lesions were observed in the left lateral ventricle on surgery. These cystic lesions were excised as much as possible. The frozen section of the cyst wall was compatible with the abscess capsule. Direct Gram staining of the surgical material showed filamentous, branching Gram-positive bacilli and moderate polymorphonuclear leukocytes (11–25 cells/ per low-power field [lpf], at 10× magnification) (Figure 2). The isolate was later identified as N. otitidiscaviarum by matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS).
Vancomycin was discontinued, and intravenous trimethoprim-sulfamethoxazole (TMP-SMX) was initiated at a dosage of 15 mg/kg/day (based on the TMP component). High-dose meropenem (2 g three times daily) was continued. The patient, with a postoperative GCS of 6, was extubated on postoperative day 12.
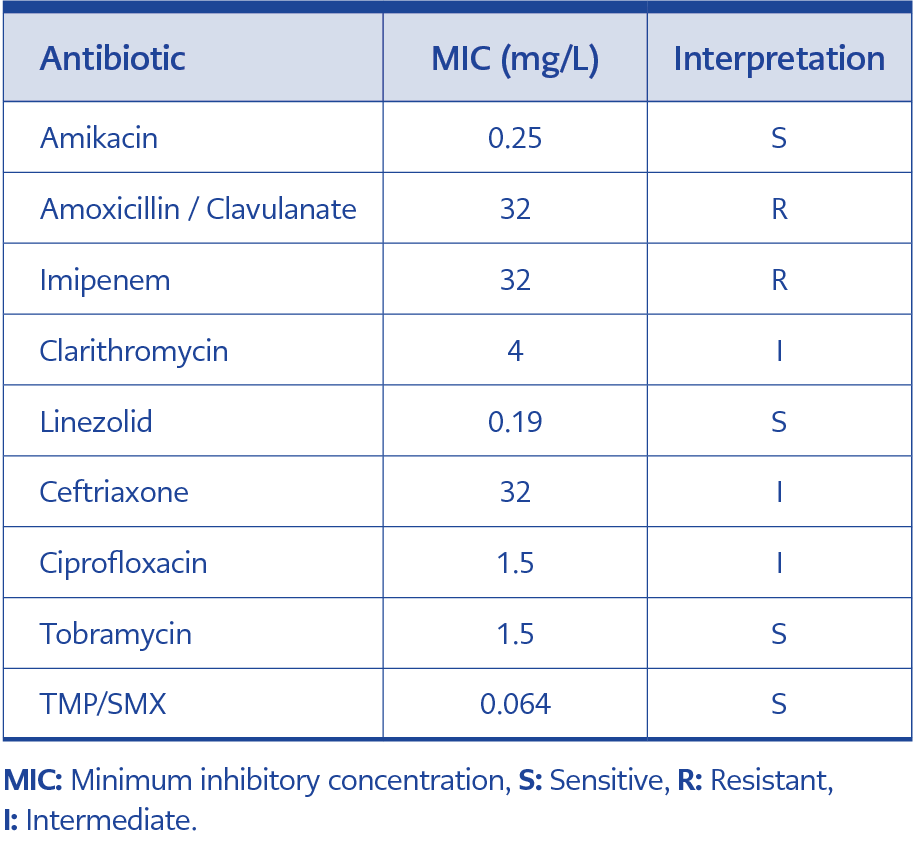
Table 1. Antimicrobial susceptibility profile of Nocardia otitidiscaviarum.
The patient’s condition deteriorated, and follow-up MRI showed disease progression. Antibiotic susceptibility testing was performed using a gradient method (bioMérieux, France) (Table 1), and test results were interpreted according to the breakpoints recommended by the Clinical and Laboratory Standards Institute (CLSI) for Nocardia and other aerobic actinomycetes (5). Based on these results, meropenem was discontinued, and intravenous linezolid was initiated at a dose of 600 mg twice daily.
The next day, the patient’s GCS declined to 3, and an external ventricular drain (EVD) was reinserted. Amikacin was added to the treatment regimen via EVD (30 mg/day). On day 38 of TMP-SMX treatment, Nocardia was no longer isolated from the CSF cultures. Despite achieving a therapeutic serum level (7.4 mg/L), linezolid was discontinued on day 10 because of thrombocytopenia (51 × 10³/µL). Following recovery, a lower dose (400 mg twice daily) was retried, but thrombocytopenia recurred within a week, requiring its cessation again.
Despite ongoing treatment with TMP-SMX and amikacin, the patient’s condition fluctuated with a GCS around 12. On the 76th day of TMP-SMX and the 30th day of amikacin therapy, the patient died because of septic shock caused by catheter-associated multidrug-resistant Klebsiella pneumoniae.
Discussion
Nocardia is an opportunistic, Gram-positive bacillus that can cause localized or systemic suppurative infections (6). Although nocardiosis primarily affects immunocompromised individuals, it can also occur in immunocompetent hosts. Among CNS infections, Nocardia most frequently causes brain abscesses; rarer manifestations include meningitis and ventriculitis (7).
Ventriculitis is an uncommon CNS infection, often secondary to trauma, hemorrhage, neurosurgery, external ventricular devices, meningitis, cerebral abscesses, or immunosuppression (4). Primary pyogenic ventriculitis, which is rare in adults, is primarily seen in immunocompromised children (8). Common pathogens include Streptococcus pneumoniae, Neisseria meningitidis, and Staphylococcus aureus (9).
Magnetic resonance imaging is the gold standard for diagnosis, showing irregular ventricular debris and other characteristic changes. The most common finding is irregular ventricular debris hyperintense compared to CSF on T1-weighted images and hypointense on T2-weighted images. In addition, hydrocephalus, periventricular hyperintense signals, ependymal enhancement, and choroidal swelling can also be detected (4,10).
Accurate identification of Nocardia spp. requires long incubation, careful microscopic examination, and appropriate media. Molecular testing (i.e., the gene encoding 16S rRNA) is the gold standard, but MALDI-TOF MS is more commonly used (6). N. otitidiscaviarum is less prevalent and pathogenic than other Nocardia spp., accounting for only 4.3% of CNS nocardiosis cases (11).
Empirical treatment for CNS nocardiosis typically includes TMP-SMX due to its good CNS penetration (12). However, susceptibility testing is crucial, as resistance patterns vary. In our case, treatment was initially with TMP-SMX and meropenem, and later adjusted to TMP-SMX, linezolid, and amikacin based on susceptibility results. When the treatment was adjusted based on the patient’s antibiotic sensitivity results, a significant improvement in the GCS was observed.
We identified five previously reported cases of Nocardia-associated ventriculitis (Table 2) (11-15). Review of reported Nocardia-associated ventriculitis cases shows that most patients were immunocompromised (e.g., corticosteroid use, alcohol dependence, malignancy). Meningitis frequently co-occurred with ventriculitis, and CSF findings were often non-diagnostic, underscoring the importance of surgical sampling and advanced microbiologic techniques (such as MALDI-TOF MS or 16S rRNA sequencing). Despite early and appropriate therapy, mortality remained high. Among fatal cases (including our patient), one involved intracranial herniation and two developed secondary bacteremia, highlighting complications and systemic infections as key determinants of poor prognosis.
Conclusion
Nocardia infections can occur in immunocompetent individuals or those with secondary immunosuppression, such as individuals using corticosteroids. Although empirical therapy for CNS infections targets common pathogens, rare organisms like Nocardia require clinical suspicion. TMP-SMX is the mainstay of treatment. A multidisciplinary approach and timely communication with the microbiology laboratory are essential for early diagnosis and appropriate management. Even with accurate diagnosis and appropriate treatment, therapeutic challenges and the emergence of secondary infections may negatively impact the clinical course and worsen the prognosis.