Introduction
Leishmaniasis is a vector-borne parasitic disease transmitted by the bite of infected female sandflies (1, 2). Leishmania species can cause various clinical manifestations, ranging in severity from spontaneously regressing cutaneous lesions to visceral disease, which is fatal in over 95% of cases if left untreated (1, 2). Visceral leishmaniasis (VL) presents unexplained prolonged fever, hepatosplenomegaly, lymphadenopathy, and cytopenia (2, 3). Bangladesh, India, Nepal, Sudan, and Brazil are the countries where VL is most common (4). Although cutaneous leishmaniasis is widespread, the incidence of VL in Türkiye is between 0.02 and 0.05 per 100,000 population (5).
Brucellosis is a zoonotic disease caused by Brucella species, which comprise Gram-negative, facultative, intracellular bacteria. Transmission to humans occurs through the consumption of infected, unpasteurized animal milk and milk products, direct contact with infected animal materials on damaged skin or mucosa, and the inhalation of infected aerosol particles (6). It is endemic in Türkiye, with an incidence of 12.32/100,000 population in 2019 (7). Human brucellosis has very different clinical presentations and is called the “great imitator,” similar to tuberculosis and syphilis (8).
Case
A 57-year-old male patient was admitted to the hematology clinic of our hospital on January 12, 2021, with fever, weakness, and night sweats. He had lost 7 kg in the month prior to his admission. There were no additional symptoms except for a dry cough. He was prescribed levocetirizine 5 mg daily for allergic rhinitis. The patient was married and lived in Zonguldak. He was a machinist and frequently traveled all over Türkiye. In epidemiological history, there was no evidence of tuberculosis, animal contact, or consumption of unpasteurized milk or cheese.
Two months earlier, he was diagnosed with COVID-19, and it had been observed that his hemoglobin (Hb) decreased to 10.6 g/dL. Additionally, his C-reactive protein (CRP) level was elevated concomitantly.
In the thoraco-abdominopelvic computed tomography (CT) performed in January 2021, splenomegaly (the anteroposterior diameter was 20 cm) was the only pathological finding. The bone marrow biopsy performed at an external center revealed no significant findings indicative of hematological malignancy.
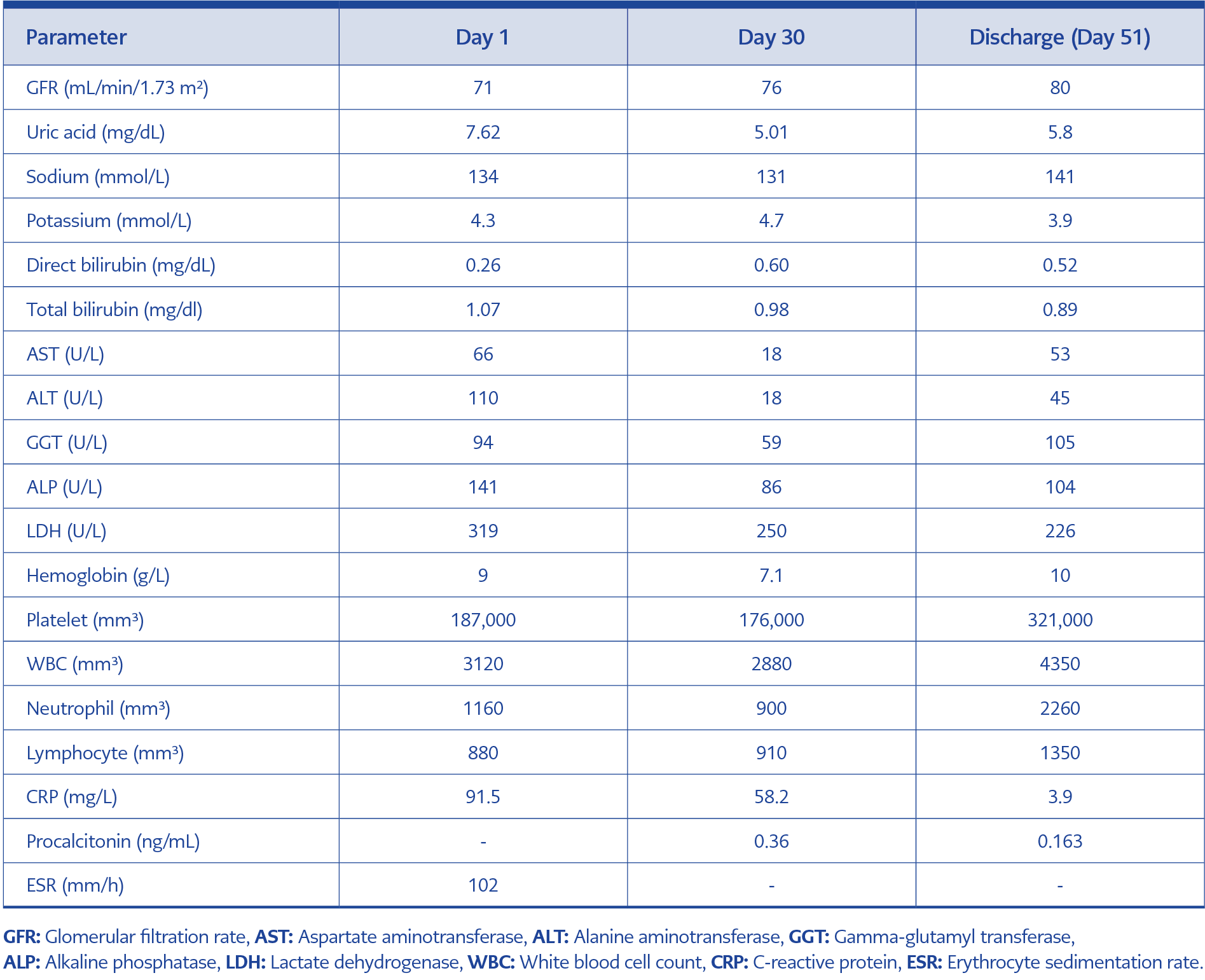
Table 1. Laboratory parameters on Day 1, Day 30, and Day 51 of hospitalization.
The patient was hospitalized in our hospital’s hematology clinic on January 22, 2021. During the physical examination, the vital signs were stable. There was hepatomegaly and splenomegaly. Laboratory tests revealed elevated liver enzymes, anemia, and leukopenia (Table 1). Anisocytosis, hypochromic erythrocytes, tear cells, and dysplastic neutrophils were observed in the peripheral smear, and no signs of hemolysis were found. The Rose Bengal test (RBT) was negative. No significant positivity was detected in rheumatological tests.
The positron emission tomography–computed tomography (PET-CT) scan report stated “splenomegaly, increase in non-homogeneous activity in the bone marrow.” Transthoracic and transesophageal echocardiograms revealed no signs of infective endocarditis.
On February 2, 2021, a new bone marrow biopsy was conducted at our center. The patient was referred to the infectious diseases service because hematological malignancy was excluded.
The RBT conducted in the infectious diseases laboratory yielded positive results. The Wright agglutination test also yielded a positive result with a titer of 1:640. The patient was diagnosed with brucellosis. Doxycycline 2 × 100 mg po and rifampicin 1 × 600 mg po were initiated. As fever and cytopenia persisted into the second week of treatment, a sacroiliac magnetic resonance imaging (MRI) was conducted on February 17, 2021, due to complications. Sacroiliitis was not observed. However, there were diffuse pathological signal changes in the medullary bone marrow density in the pelvic structures, suggestive of hematological diseases. In the patient’s second bone marrow biopsy, no signs of neoplasia were found; 70% hypercellular bone marrow with polytypic immunoglobulin G (IgG) was noted.
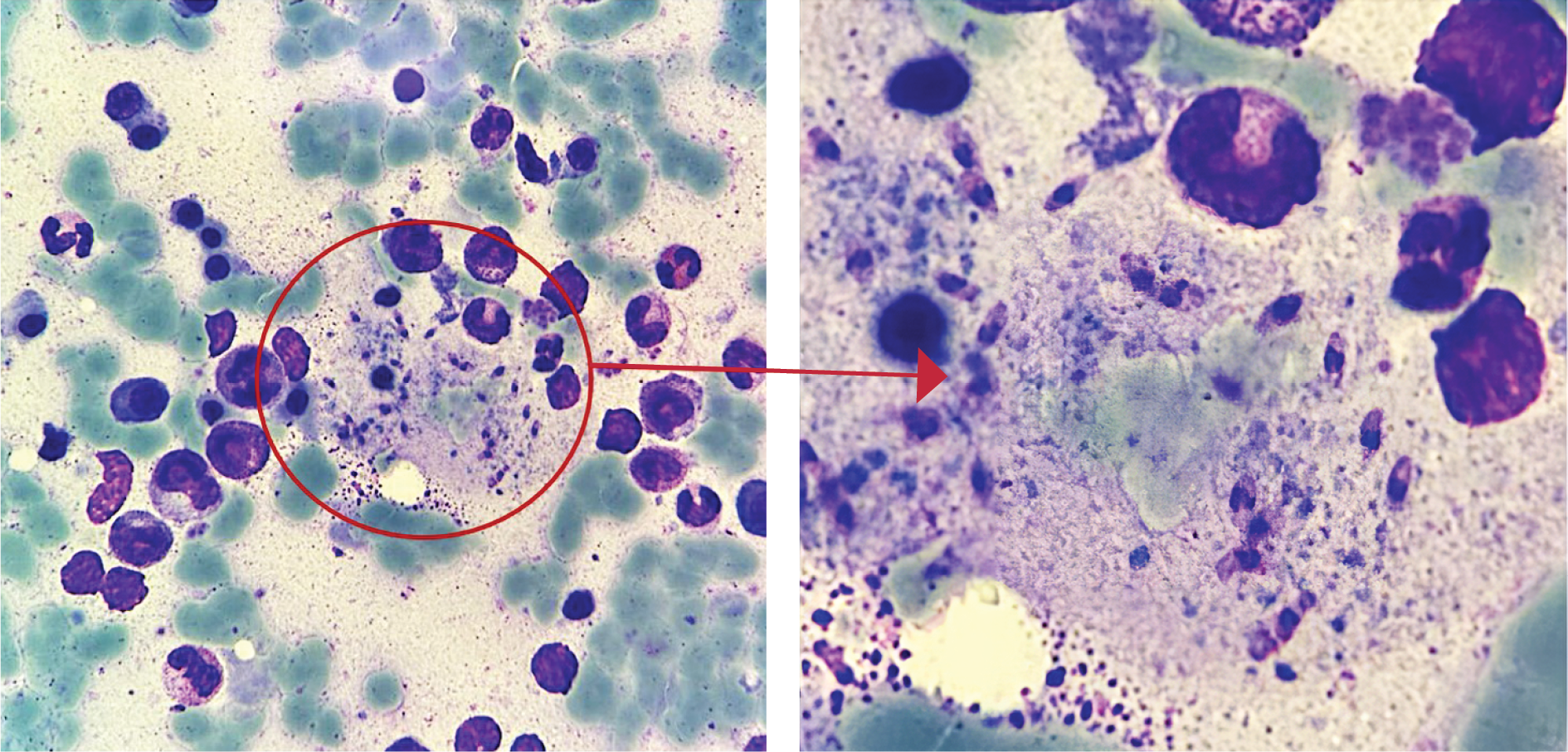
Figure 1. Leishmania bodies are seen in macrophages in the bone marrow aspiration smear.
The patient’s peripheral blood smear was examined by pathology based on his MRI results, which indicated persistent cytopenia. During the evaluation, granulocyte predominance was observed, and no obvious parasites were detected; however, some suspicious degenerated cells, as well as platelets, were detected. Upon re-evaluating the bone marrow biopsy for parasites, a focus consistent with Leishmania was observed in the background. The microorganisms were identified as sparse and scattered amastigote forms, some exhibiting enlarged cytoplasm, nuclei, and partially discernible kinetoplasts (Figure 1). Leishmania PCR testing on blood samples sent to the National Parasitology Reference Laboratory of the General Directorate of Public Health yielded a positive result.
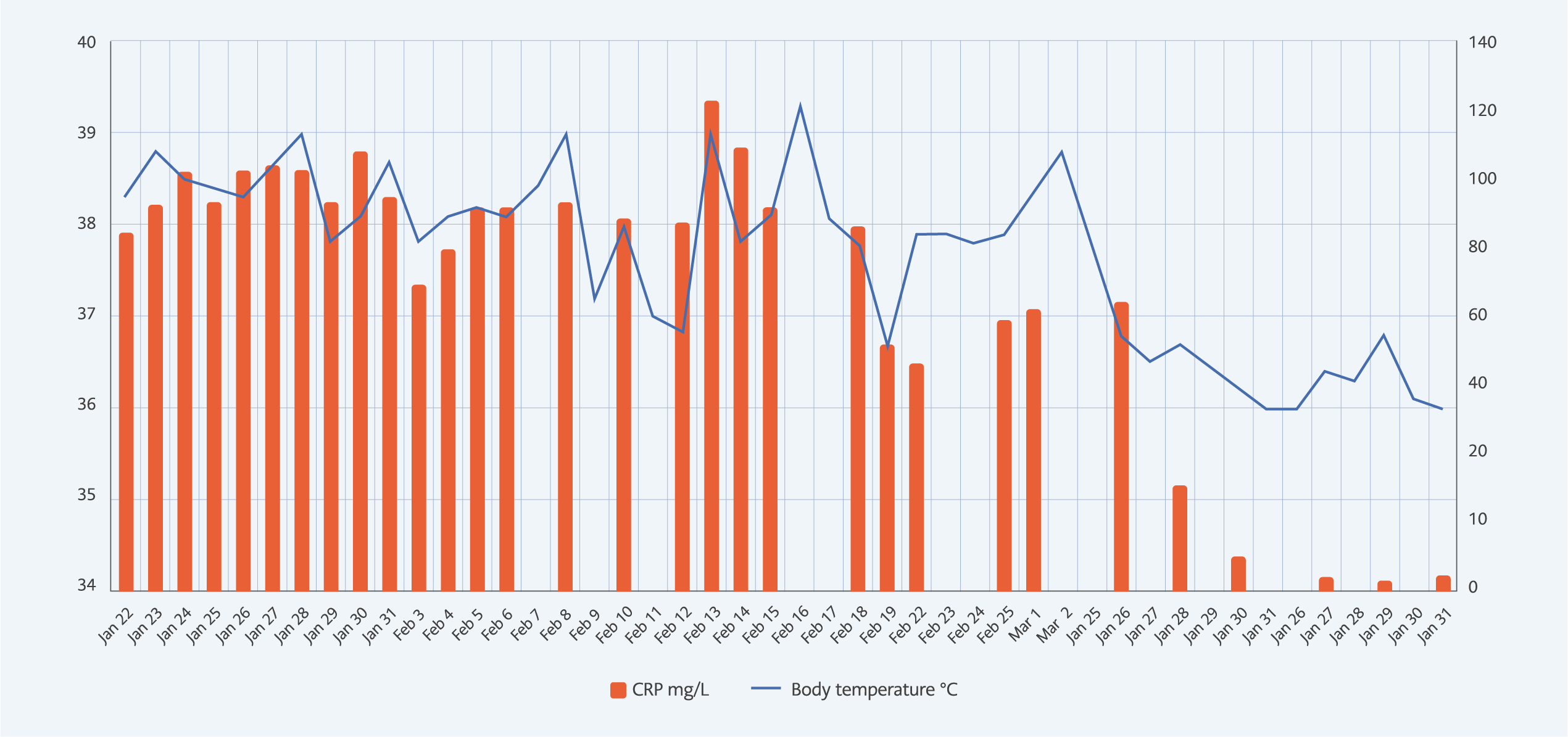
Figure 2. C-reactive protein and body temperature values monitored during the patient’s hospitalization.
The patient, whose fever persisted on the 24th day of brucellosis treatment, was diagnosed with VL, and liposomal amphotericin B 240 mg IV daily was initiated. On the third day of treatment, both fever and CRP began to decrease (see Figure 2). Upon completion of the 14-day treatment, the cytopenia resolved. Except for right cephalic vein thrombosis, which appeared on Day 10, no amphotericin B-related side effects were observed.
After a 14-day course of VL treatment, the patient was discharged on the 38th day of brucellosis treatment. During outpatient follow-up, doxycycline and rifampicin were completed for six weeks.
Discussion
Even though VL is becoming less common worldwide, it still affects developing countries (9). In Türkiye, the most common type is Leishmania infantum MON-1, which is found in the Aegean and Mediterranean regions (10). The World Health Organization (WHO) statistics indicate that 48–64% of VL cases reported from Türkiye were individuals older than 14 years in 2018 (5). Early diagnosis and treatment are crucial because of the high mortality rate in untreated cases. Classical diagnosis is achieved by observing amastigotes during microscopic examination of tissue samples or cultures and is not always straightforward (2). Our patient underwent two bone marrow biopsies and many microscopic examinations, and the diagnosis was confirmed with the third one. In the literature, the sensitivity of tissue examination is >90% in the spleen, 50–80% in the bone marrow, and lower in lymph node examinations (1). With more locations and longer examination times, sensitivity increases (11).
Brucellosis is endemic in Türkiye. In cases like ours, which present with B symptoms, cytopenia, and elevated liver enzymes, it must be investigated. The sensitivity of RBT ranges from 90% to 100% in studies and is recommended as a rapid diagnostic test (7, 8). Although false positives are common, false negatives are rare (8). False-negative results may occur due to early incubation of the disease or a small clump size in serum with low antibody titers (12).
In our case, the fact that the first RBT was negative and the second was positive may be associated with increased antibody titers. We diagnosed brucellosis with serology, but the gold standard method is culture. We consider the possibility of false positivity in serology because of VL; however, cross-reactivity is observed between Brucella spp. and many Gram-negative bacteria. There is no data supporting cross-reactivity with Leishmania spp.
Visceral leishmaniasis and brucellosis are infections that can occur independently in Türkiye. However, coinfection is rare. Upon reviewing the literature, we found a total of three cases of coinfection, one pediatric and one with a possible diagnosis of VL (13-15).
To the best of our knowledge, this is the second reported adult case in the literature with the proven co-infection of VL and brucellosis. Among these cases, including ours, in those diagnosed with VL by pathology, the brucellosis diagnosis was made serologically. In the case of possible VL and Brucella melitensis coinfection from Sudan,
B. melitensis was cultured, and VL diagnosis was confirmed only by direct agglutination test (15). These data indicate the possibility of cross-reactivity between Brucella spp. and Leishmania spp. However, in this context, serological studies are required in endemic areas.
Conclusion
There is a case of VL and brucellosis coinfection that presented with B symptoms and cytopenia, which had difficulty diagnosing with two bone marrow biopsies. Particularly in regions where they are endemic, VL and brucellosis should be considered in the differential diagnosis of hematologic malignancies, and pathology specimens should be assessed with this consideration in mind. In cases where there is a strong suspicion of VL but a definitive diagnosis cannot be established, a spleen aspiration may be considered, given the high risk of complications. This is due to the relatively lower diagnostic value of lymph nodes and bone marrow biopsies in such cases. Other serological methods can also be used.