Introduction
Parvovirus B19 (PVB19) is a single-stranded DNA virus belonging to the family Parvoviridae (1). It can cause erythema infectiosum, arthropathies, aplastic crisis, immune-mediated rash, and arthritis. Dermatological manifestations of acute PVB19 infection include vesiculopustular rash, petechiae, purpura, glove sock syndrome, leukocytoclastic vasculitis (LCV), polyarteritis nodosa, and Henoch-Schönlein purpura (2). In normal individuals, hematological findings may also include mild and transient anemia, leukopenia, and thrombocytopenia (1). Here, we report a case of LCV in an immunocompetent host with a high probability of association with PVB19.
Case
A 26-year-old woman was admitted to the infection disease department with a 10-day history of fever, fatigue, rash, and edema on the hands and feet. She was a nurse in a hospital. Her complaints started with fever, sore throat, and muscle and joint pains after going to a picnic with children. A week later, a rash developed on her ankle. The rash spread to the thighs and upper extremities. She had no other complaints, history of medication, substance use, transfusion, or additional disease. At the admission, the temperature was 37.3°C, blood pressure was 100/70 mmHg, and pulse rate was 105/minute. On physical examination, the tonsils were hyperemic and hypertrophic. There were multiple erythematous, maculopapular, and pruritic rashes on the upper and lower extremities. Other system examinations were normal. Laboratory findings included hemoglobin 13 g/dL, leukocyte count 11,500 /mm³, platelet count 315,000 /mm³, eosinophils 16%, and D-dimer 3990 µg/L. The erythrocyte sedimentation rate was 21 mm/hour, and C-reactive protein was 59 mg/dL (0–5 mg/dL). Other laboratory tests were normal.
The nasopharynx, blood, urine, and stool cultures were negative. The respiratory multiplex polymerase chain reaction (PCR) test was negative. Serology results for hepatitis A, hepatitis B, hepatitis C, syphilis, Brucella, HIV, Epstein-Barr virus, and cytomegalovirus were negative. PVB19 IgM test had a borderline value, whereas PVB19 IgG was negative via an enzyme-linked immunosorbent assay (ELISA). A skin biopsy was performed with the preliminary diagnosis of cutaneous LCV, pityriasis lichenoides et varioliformis acuta (PLEVA), psoriasis vulgaris, and lichen planus.

Figure 1. Purpuric maculopapular lesions on the lower extremities.
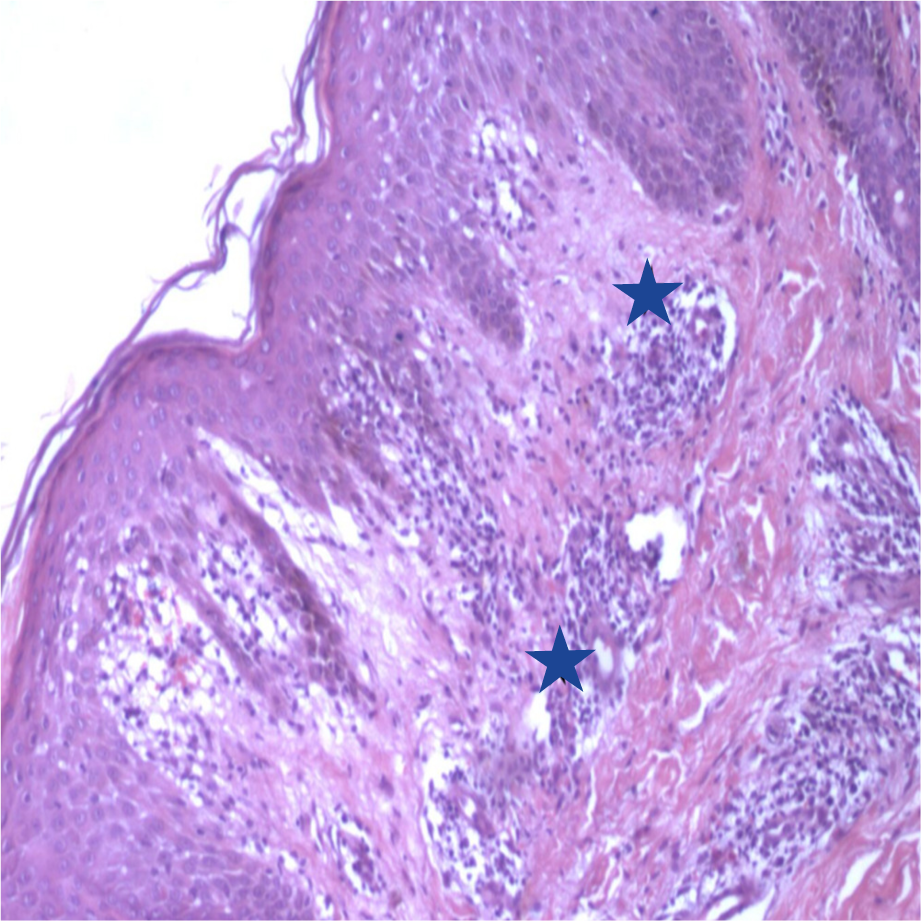
Figure 2. Perivascular eosinophilic and neutrophilic infiltration.
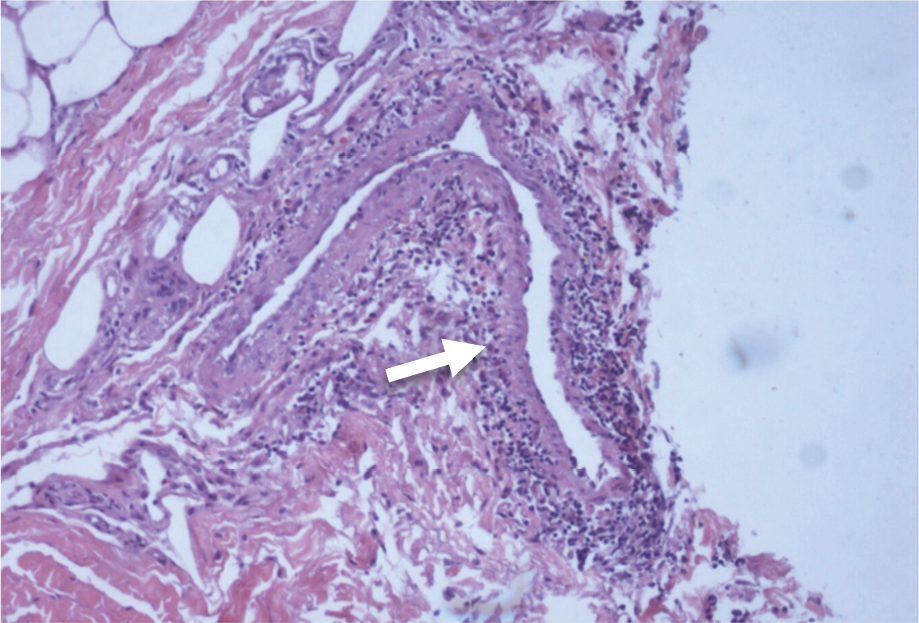
Figure 3. Polymorphonuclear infiltration of the venous vessel wall.
Her fever continued, and her rashes spread (Figure 1). Biopsy revealed ‘perivascular inflammation with perivascular eosinophils and infiltration with eosinophils and polymorphonuclear leucocytes infiltrating the walls of venous vessels’ (Figure 2 and Figure 3). IgA, IgG, IgM, complement 3, and fibrinogen were not stained by direct immunofluorescence. The pathology result was ‘LCV’. Autoimmune and tumor markers were negative. Thorax computed tomography and abdominal and urinary ultrasonography were normal.
On day 10, her hemoglobin level decreased to 9.6 g/dL, and her platelet count decreased to 234,000 /mm³. Intravenous (IV) methylprednisolone 60 mg/day was initiated upon diagnosis of transient aplastic crisis. Arthralgia, rash, and edema regressed. PVB19 DNA was tested in serum using PCR, and the result was negative. On day 14, serological tests were repeated upon clinical suspicion. It was found that the IgM antibody titers increased >4-fold, and the IgG test changed from negative to positive (seroconversion). Based on these findings, vasculitis was thought to be related to PVB19 infection. Her rashes regressed on the fifth day of treatment; her fever and blood levels normalized.
Discussion
Although PVB19 is common in childhood, it can also be seen in naive adults. The cases increase in spring and summer (1, 3). Our patient was admitted in June. Transmission is mainly by droplets and occurs from children to adults (1). PVB19 infection can cause nosocomial outbreaks with a high attack rate among healthcare professionals (4, 5). The mode of transmission of PVB19 was not elucidated in our case because the patient was both a nurse and had contact with children.
Considering the 120-day erythrocyte lifespan, PVB19 causes no clinically significant decrease in erythroid precursor cells (1). Nevertheless, PVB19 was related to severe aplastic anemia in previously healthy adults in a few reported cases (6, 7). In our case, although no aplastic anemia required transfusion, the hemoglobin level dropped from 13 g/dL to 9.6 g/dL. PVB19 infection is associated with polymorphic skin manifestations in adults. Mage et al. (2) showed that erythematous (86%) and purpuric (69%) lesions were the most common skin involvements. Pruritus was observed in almost half (48%) of the patients. The frequency of rashes was found on the legs (93%), trunk (55%), arms (45%), and face (20%). In adults, the rash is less pronounced than in children and usually appears on the legs, trunk, and arms (1, 3, 8). In children, the skin manifestation is typically a rash that looks like a slapped cheek. In one study, the incidence of erythema on the cheeks was 89% in children and 20% in adults (8). In line with the literature, our patient had erythematous and pruritic rashes on the legs and arms, with no lesions on the face, neck, or trunk.
Past infection is determined by detecting IgG antibodies, while acute infection can be deduced by the presence of IgM. Among immunocompromised patients, detection of B19V DNA may be beneficial because of a deficiency in antibody production. The possible persistence of B19V in blood (viremia) also among immunocompetent subjects greatly complicates the interpretation of PCR positivity. Serological tests and PVB19 PCR should be used complementarily in patients with clinical findings and should be interpreted together (9). In the absence of antibodies, repeat serology is required after two weeks (10). In our case, although IgM was at a borderline value, and PVB19 PCR and IgG were negative, we repeated the tests two weeks later due to high clinical suspicion. We diagnosed the patient with a >4-fold increase in IgM titer and IgG seroconversion in serology.
In the presence of vasculitis, systemic steroid use is beneficial. Nevertheless, there is no consensus about the dose and duration of steroid treatment in the literature. Rodríguez Bandera et al. (3) used tapering doses of prednisone, starting at 0.5 mg/kg/d, with reductions of 10 mg every 10 days for patients with PVB19-related LCV. In two PVB19-related LCV cases reported by Crowson et al. (11), steroids were used, but no information was provided on the dose and duration. Our patient responded to five days of IV methylprednisolone 60 mg/day. Some patients diagnosed with LCV recovered without treatment (12, 13). In one study, while PVB19 infection was self-limiting in 75.5% of patients, systemic corticosteroids relieved symptoms in 20% of cases (3). A blood transfusion may be required for the aplastic crisis. Short-term intravenous immunoglobulin (IVIG) therapy can be effective in immunocompromised patients with pure red cell aplasia related to PVB19 (14). Intravenous immunoglobulin was not needed in our patient, and the disease was self-limited with short-term steroid use.
PVB19-related LCV cases have occasionally been reported in children but are rare in adults. PVB19 has been associated with vasculitis, such as polyarteritis nodosa, Wegener’s granulomatosis, and cutaneous LCV (2, 3, 12, 13, 15-17). IgA deposition and renal involvement were observed in most adult patients with PVB19-related LCV (2, 12, 13, 17). Discrepantly, IgA deposition and renal involvement were not observed on biopsy in our patient. Our patient was a rare case of an immunocompetent adult diagnosed with LCV without other systemic involvement. Our patient was the first case of PVB19-related LCV reported from Türkiye in an immunocompetent adult patient.
In conclusion, the >4-fold increase in IgM titer in a two-week interval, the development of IgG seroconversion, and the absence of other vasculitis-associated factors are consistent with a causal role of PVB19 when evaluated with anamnesis and clinic. In a young adult presenting with fever and rash, PVB19 should be kept in mind, and serological borderline values should be repeated in case of clinical suspicion.