Introduction
With the reports of patients with mpox (formerly monkeypox) outside Africa in April 2022, a second epidemic fear emerged around the world following the coronavirus disease 2019. From the onset of the mpox outbreak as of December 25, 2022, 21,055 human mpox virus cases were reported from 29 European countries, 63 from Turkey, and three from Western Balkan countries (1).
Mpox infection typically presents with fever, rash, and swollen lymph nodes and may lead to several medical complications (2). The infection usually spreads through prolonged skin-to-skin contact and shared objects, including towels, clothes, and sheets, or respiratory secretions. Whether human immunodeficiency virus (HIV) infection increases the likelihood of contracting mpox infection is unknown (3, 4). Mpox has been reported mainly, but not exclusively, among men who have sex with men; however, anyone having close contact with an infected person is likely to contract mpox regardless of the type of sexual intercourse (5). Herein, we described four patients with mpox, three HIV-positive and one HIV-negative.
Case Presentation
Case 1

Figure 1. Several umbilicated pustules on the penis in Case 1. (a) Initial presentation of a skin lesion on the third day. (b) The lesions with central scabbing on the 10th day. (c) The lesions on the 14th day.
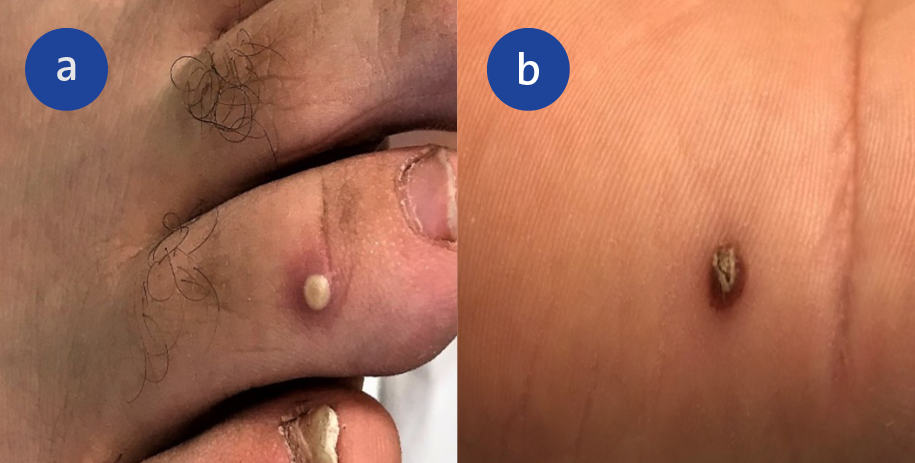
Figure 2. Hand and foot lesions in Case 1. Pustular umbilicated rash on the right toe (a) and palm (b) in the second week.
A 37-year-old male patient was admitted to the hospital with a rash in the genital area (Figure 1). The patient had a fever, headache, myalgia, and diarrhea one day before the lesions occurred. The rash first appeared in the penile area and then spread to the lower extremities, feet, trunk, hands, ears, and scalp (Figure 2). The lesions were numerous umbilicated pustules that clustered. Also, right inguinal lymphadenopathy was presented. He was prescribed valacyclovir for presumed varicella-zoster virus infection, but the number of lesions increased. He had a history of diabetes mellitus type I and urogenital surgery 11 days ago. He had no history of close sexual contact with an infected person but a history of sharing bathrooms and towels at work. The patient underwent testing for HIV and syphilis, which were negative. The swabs from the lesions and oropharynx were obtained for the mpox virus. The mpox polymerase chain reaction (PCR) test was positive for the lesions.
He was admitted to the hospital on the 12th day of his illness and examined daily for new skin lesions. Although fourteen days had passed since the initial appearance of lesions, new lesions appeared. Lesions crusted approximately 21 days after the first appearance, and the patient recovered.
Case 2
A 37-year-old man was admitted to the hospital with anal pain. He complained of high fever, anal pain, and lesions in the perianal region. The lesions appeared 1-2 days after the fever began. Because mpox disease was not initially suspected, a general surgery physician diagnosed him with an anal abscess and prescribed amoxicillin-clavulanate. After three days of treatment, his fever regressed. However, umbilicated pustular lesions increased in the anal region. He reported protected receptive anal intercourse 20 days ago with a casual partner. In 2019, he was diagnosed with HIV. He had been taking bictegravir/emtricitabine/tenofovir alafenamide (BIC/FTC/TAF) for three years. His CD4+ lymphocyte count was 376 cells/μL, and the HIV RNA was <20 copies/mL.
His physical examination revealed two lesions in the penile region and many umbilicated pustular lesions in the perianal region. Swabs were taken from the oropharynx and anal lesions for a PCR test, and the swab from the anal lesions tested positive for mpox. He was hospitalized on the ninth day of his illness due to proctitis. On the third day of hospitalization, his rash had crusted, and his anal pain had subsided.
Case 3
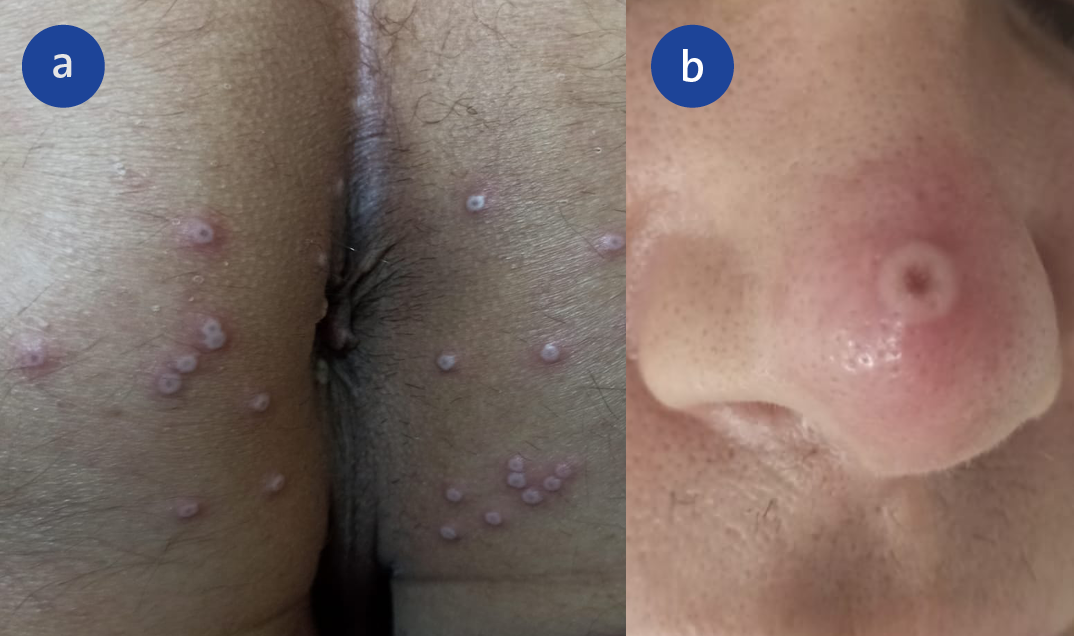
Figure 3. Mpox skin lesions in the different areas in Case 3. (a) Perianal umbilicated pustules on the third day of lesions. (b) A umbilicate pustule with necrotic crust and erythematous halo on the nose six days after lesions appear.
A 41-year-old male patient was admitted to our clinic with complaints of pain in the bilateral inguinal area and painful, itchy, umbilicated papules in the perianal region for three days (Figure 3a). He had a fever, cough, weakness, and headache that started three days before the rash. He reported that he had protected receptive anal intercourse with multiple partners five days before his complaints. The patient had an HIV infection in 2019. He was under treatment with BIC/FTC/TAF and had a good virologic and immunological response (CD4+ lymphocyte count=1035 cell/μL; HIV-RNA <20 copy/mL). He also had ankylosing spondylitis for 15 years but had not received immunosuppressive therapy.
Physical examination revealed bilateral painful inguinal lymphadenopathy and perianal umbilicated pustules. The swabs from the lesions and oropharynx tested PCR-positive for the mpox virus, and the patient was hospitalized. He had a fever for one day after hospitalization, and a new lesion appeared on his nose (Figure 3b). The patient was discharged and encouraged to maintain home quarantine for at least 21 days. By day 16, the lesions were completely healed, and he recovered without any complications.
Case 4
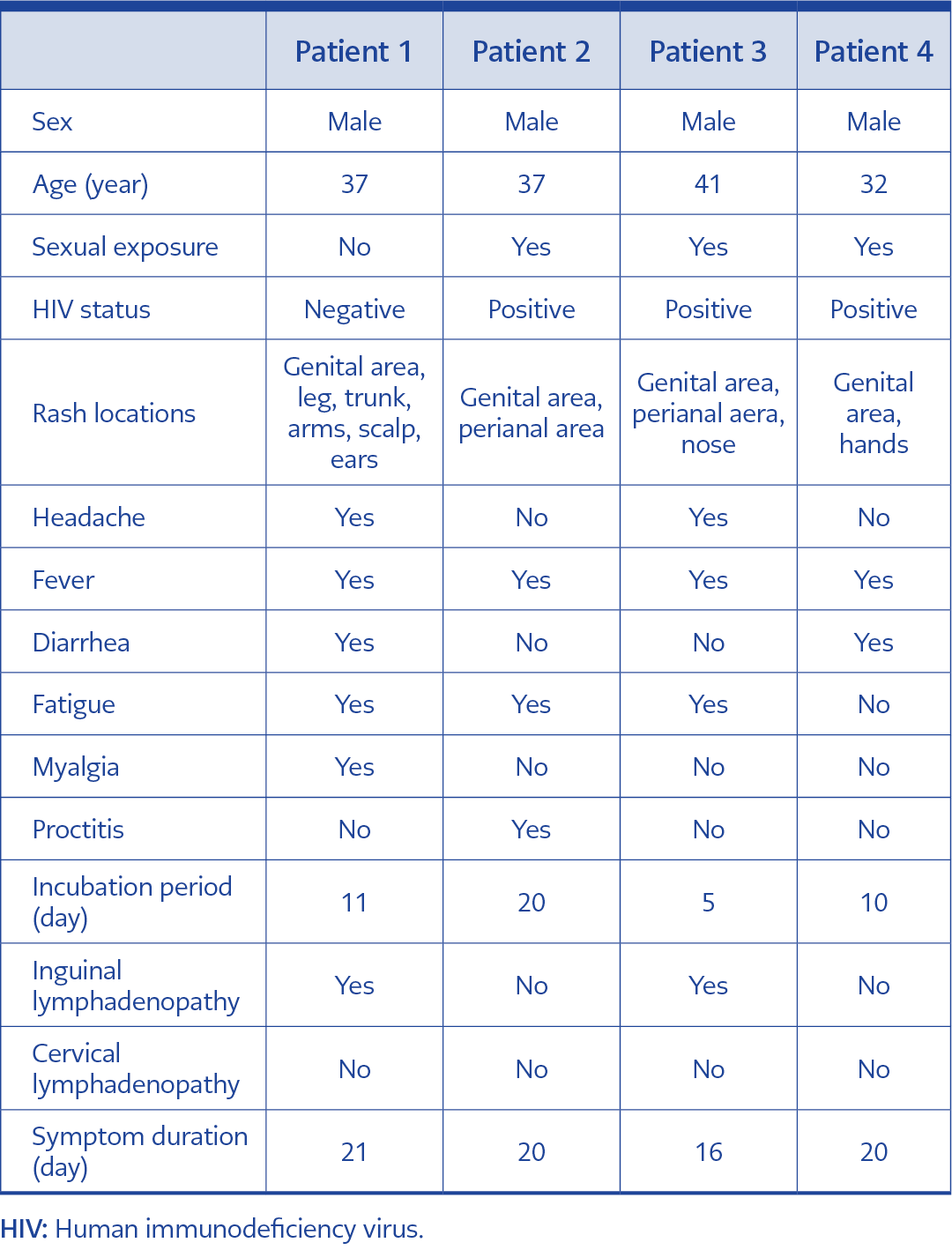
Table 1. Characteristics of demographic and clinical data of the patients with mpox.
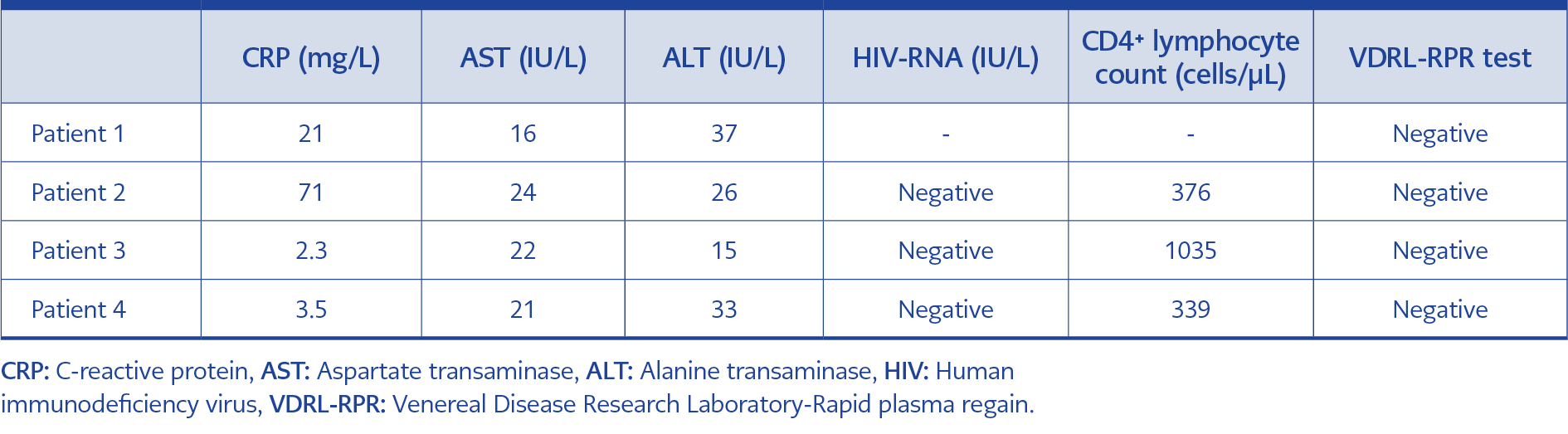
Table 2. Characteristics of laboratory data of the patients with mpox.
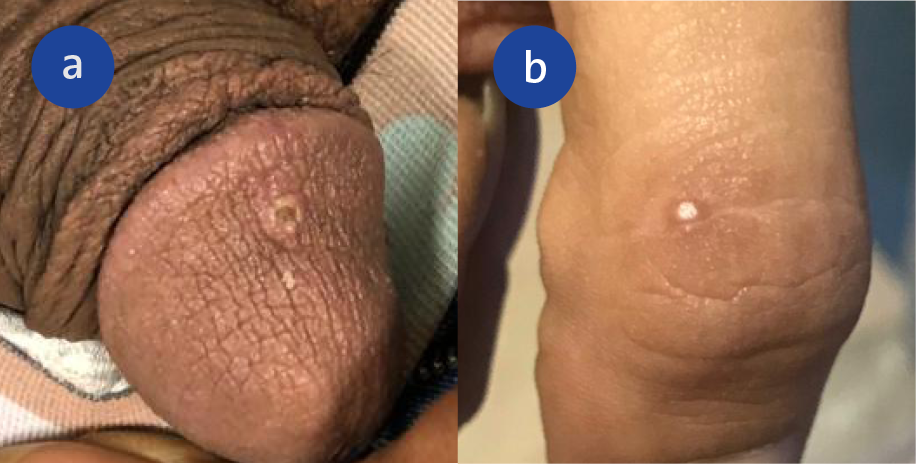
Figure 4. A papular rash on the penis (a) and the right finger (b) on the third day of lesions in Case 4.
A 32-year-old male patient was admitted to our clinic with complaints of genital skin lesions. The patient had a fever, diarrhea, sore throat, and body ache for three days before the skin lesions. He engaged in condom-free sexual activity and had sexual contact with a male ten days before the onset of symptoms. The patient had received BIC/FTC/TAF for two years because of the diagnosis of HIV infection. His CD4+ lymphocyte count was 339 cells/μL, and the HIV RNA was <20 copies/mL. The physical examination demonstrated one papule on the glans penis and another on the right finger filled with a white fluid, overlying erythematous skin (Figure 4). He had no lymphadenopathy. The lesions tested PCR-positive for the mpox virus. In twenty days, the lesions completely disappeared, and no new lesions were observed after that. The demographic, clinical, and laboratory data of all patients are presented in Tables 1 and 2.
Discussion
This report presented four cases of mpox virus infection followed in a single center in Turkey. The cases had no history of international travel or contact with a confirmed person with mpox, as in the current epidemic (6). Although mpox infection can affect anyone, bisexual men and men who have sex with men are more likely to be affected by this epidemic (7). In this case series, three were men who had sex with men and who had had recent sexual contact. The remaining patient (Case 1) had no history of sexual contact, but he reported using shared bathrooms and towels at work. Therefore, it was believed that contamination could have originated in the workplace. Sharing bathrooms and personal items in close quarters have been reported as a significant transmission mode. (8).
This outbreak is characterized by lesions more limited to the genital and perianal area, with minor or non-systemic symptoms (9). The lesions in the second case were limited to the anogenital area, and his anal abscess healed in a short time without complications; however, a severe case that required a colostomy was reported in Turkey (10).
Although it is known that the skin lesions are typically seen at the same stage in mpox disease, they can also be seen at different stages, as in the first case (9, 11, 12). All our cases had prodromal symptoms such as short-term fever, myalgia, or fatigue, followed by a vesicular-pustular rash that began in the genital area and, in some cases, spread to the rest of the body. The clinical presentation was more complex in the first two cases because the first one had a rash in more areas, such as the genital area, face, trunk, and extremities, and the second had proctitis. On the other hand, we diagnosed the later cases more quickly due to the experience from the first cases.
The incubation period of mpox virus infection can vary from 3 to 21 days (13). In our cases, the mean incubation period was 11 days. While the third case’s incubation period was five days, the symptoms of the second case occurred on the twentieth day. Mpox virus infection is a generally self-limiting disease (14, 15). Although most of our cases were people living with HIV, they had mild diseases. There is limited information on people living with HIV and mpox virus. However, it appears that those with a CD4+ lymphocyte count of fewer than 200 cells/μL, persistent viremia (>200 copies/mL), or a recent HIV-related disease should be considered at higher risk (16). In this report, our three patients living with HIV had suppressed viremia, and their CD4+ lymphocyte count was over 200 cells/μL (Table 2). All our cases recovered without complications. Because mpox virus infection is a rare disease in Turkey (10), it may not initially be considered in the differential diagnosis of a patient with a rash. Individuals with pustular umbilicated lesions and a history of risky sexual behavior should be considered.
As with other viral infections, mpox virus infection may present with fever, myalgia, diarrhea, fatigue, and lymphadenopathy before the rash, which may lead to a delay in the diagnosis. In addition, although the disease has been reported at a high rate in certain high-risk groups, such as men who have recently had sex with men, it has also been observed in populations that have not been previously documented. Consequently, healthcare professionals must be aware of mpox cases in order to control the epidemic.